In a trio of studies published Sunday, scientists reported that they reversed aging in the muscles and brains of old mice — simply by running the blood of young mice through their veins.
The papers, from two independent groups in Cambridge and California, used different approaches to begin to unravel the rejuvenating effects of young animals’ blood, in the hopes of eventually developing a therapy that could be tested in people.
Researchers at Harvard University administered a protein found in young blood to older mice, and found that treated mice could run longer on a treadmill and had more branching blood vessels in their brains than untreated mice. A group led by a University of California, San Francisco researcher identified a molecular switch in a memory center of the brain that appears to be turned on by blood from young mice.
“These are the tissues that are really affected by advancing age. Changes in these tissues are responsible for the changes that people worry about the most — loss of cognition and loss of independent function,” said Amy Wagers, a professor of stem cell and regenerative biology at Harvard University involved in two of the studies.
Wagers said many questions remain about the mechanism of the protein and what the best therapeutic strategy might be, but she is already working to commercialize the protein discovery. The same substance is found in human blood.
Outside scientists cautioned that the findings are limited to one strain of mice and that it is not yet clear that something so simple would have dramatic anti-aging effects in people.
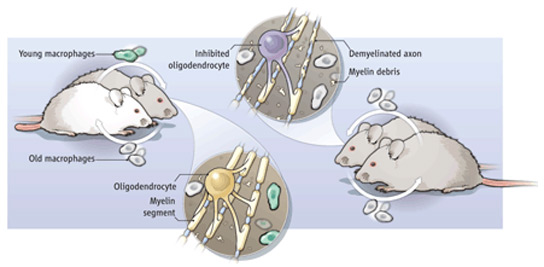
The new studies build on a decade of research that showed that young blood can have a rejuvenating effect on older mice. When scientists stitched together the circulatory systems of pairs of old and young mice, in a procedure called parabiosis, they found beneficial effects on the cells of the spinal cord, muscles, brain, and liver of the older animals. The next question was why — which of the many substances floating around in blood were responsible for the changes, and how did it work?
Last year, Wagers and another Harvard stem cell scientist, Dr. Richard T. Lee, found that a protein called GDF11 could cause a mouse heart thickened with age to revert to a youthful state. No one knew, however, whether the effect was specific to the heart, or would apply to aging in other tissues. Two of the new papers, published online by the journal Science, extend that work to the mouse brain and muscle.
In one study, Wagers and colleagues first connected the blood vessels of old and young mice. They measured profound changes to muscle stem cells in the older mice that made the cells appear more youthful. There were also changes to the structure of muscle. Next, they injected the protein that had been shown to rejuvenate hearts into the older mice. Although some individual mice did not change much, on average, the treated mice could run nearly twice as long on a treadmill as older mice not given the protein. The protein had no effect when injected into younger mice.
In a second study, Dr. Lee Rubin, director of translational medicine at the Harvard Stem Cell Institute, found that after parabiosis, the older mice had an increase in the branching network of blood vessels in the brain and in the rate of creation of new brain cells. Treated mice were more sensitive to changes in smell, suggesting the new neurons had an effect on their abilities. The GDF11 protein alone resulted in similar structural changes.
Wagers said that she has begun working with Atlas Venture, a venture capital firm based in Cambridge, to come up with a strategy to turn the insights about GDF11 into potential treatments that could be tested in people.
David Harrison, an aging researcher at Jackson Laboratory, a nonprofit research organization based in Bar Harbor, Maine, who was not involved in the research, said that an important caveat about the research is that it was done on a particular strain of mouse that is inbred. It will be important, he said, to test the protein’s effect in a more genetically diverse population of mice before thinking about extending the work to clinical trials.
Thomas Rando, a professor of neurology at Stanford University School of Medicine who pioneered using the parabiosis technique to study aging, said it is important to try and understand how young blood has its potent effects. But he said it seems very unlikely, given how complex aging is, that reversing it will depend on a single pathway.
“My answer always was and always will be there’s no way there’s a factor,” Rando said. “There are going to be hundreds of factors.”
In the third study published in the journal Nature Medicine, researchers from the University of California, San Francisco and Stanford used parabiosis to search for changes in gene activity in the brain that might help point to how young blood had its effects. They found changes in the activity of genes involved in the connectivity of brain cells in the hippocampus, a memory center.
Instead of using a specific protein, the researchers then gave older mice repeated transfusions of blood from young mice and found that the older animals improved on specific age-related memory tasks, such as locating an underwater platform and remembering an environment where they had experienced an unpleasant foot shock.
Saul Villeda, a UCSF faculty fellow who led the work, said that the results of the three studies reinforce one another, but they differ in their approach.
“I’m really interested to see whether GDF11 accounts for everything, or whether it’s going to be a combination of factors that together that has the full effect,” Villeda said.
All the researchers warned that people hoping to reverse aging shouldn’t get any wild ideas about infusing themselves with young blood, although they acknowledged making their share of vampire jokes.
“I am the oldest member of the team here, and I personally understand the sentiment for patients,” Rubin said. But he still wouldn’t try it.
Written by Carolyn Y. Johnson, who can be reached at cjohnson@globe.com. Follow her on Twitter @carolynyjohnson.
Thanks to Da Brayn for bringing this to the attention of the It’s Interesting community