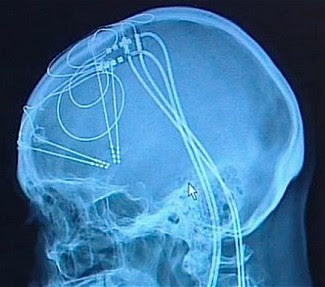
Researchers at University of South Carolina (USC) and Wake Forest Baptist Medical Center have developed a brain prosthesis that is designed to help individuals suffering from memory loss.
The prosthesis, which includes a small array of electrodes implanted into the brain, has performed well in laboratory testing in animals and is currently being evaluated in human patients.
Designed originally at USC and tested at Wake Forest Baptist, the device builds on decades of research by Ted Berger and relies on a new algorithm created by Dong Song, both of the USC Viterbi School of Engineering. The development also builds on more than a decade of collaboration with Sam Deadwyler and Robert Hampson of the Department of Physiology & Pharmacology of Wake Forest Baptist who have collected the neural data used to construct the models and algorithms.
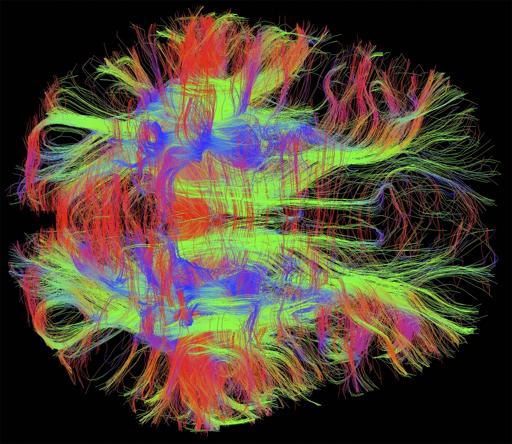
When your brain receives the sensory input, it creates a memory in the form of a complex electrical signal that travels through multiple regions of the hippocampus, the memory center of the brain. At each region, the signal is re-encoded until it reaches the final region as a wholly different signal that is sent off for long-term storage.
If there’s damage at any region that prevents this translation, then there is the possibility that long-term memory will not be formed. That’s why an individual with hippocampal damage (for example, due to Alzheimer’s disease) can recall events from a long time ago – things that were already translated into long-term memories before the brain damage occurred – but have difficulty forming new long-term memories.
Song and Berger found a way to accurately mimic how a memory is translated from short-term memory into long-term memory, using data obtained by Deadwyler and Hampson, first from animals, and then from humans. Their prosthesis is designed to bypass a damaged hippocampal section and provide the next region with the correctly translated memory.
That’s despite the fact that there is currently no way of “reading” a memory just by looking at its electrical signal.
“It’s like being able to translate from Spanish to French without being able to understand either language,” Berger said.
Their research was presented at the 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society in Milan on August 27, 2015.
The effectiveness of the model was tested by the USC and Wake Forest Baptist teams. With the permission of patients who had electrodes implanted in their hippocampi to treat chronic seizures, Hampson and Deadwyler read the electrical signals created during memory formation at two regions of the hippocampus, then sent that information to Song and Berger to construct the model. The team then fed those signals into the model and read how the signals generated from the first region of the hippocampus were translated into signals generated by the second region of the hippocampus.
In hundreds of trials conducted with nine patients, the algorithm accurately predicted how the signals would be translated with about 90 percent accuracy.
“Being able to predict neural signals with the USC model suggests that it can be used to design a device to support or replace the function of a damaged part of the brain,” Hampson said.
Next, the team will attempt to send the translated signal back into the brain of a patient with damage at one of the regions in order to try to bypass the damage and enable the formation of an accurate long-term memory.
http://medicalxpress.com/news/2015-09-scientists-bypass-brain-re-encoding-memories.html#nRlv