Researchers from Case Western Reserve University School of Medicine, University Hospitals Cleveland Medical Center (UH), Cleveland Clinic and Lifebanc (a Northeast Ohio organ-procurement organization) have developed a new way to preserve donated kidneys–a method that could extend the number and quality of kidneys available for transplant, saving more people with end-stage renal disease, more commonly known as “kidney failure.”
The team identified a drug–ethyl nitrite–that could be added to the preservation fluid to generate tiny molecules called S-nitrosothiols (SNOs), which regulate tissue-oxygen delivery. This, in turn, restored flow-through and reduced resistance within the kidney. Higher flow-rates and lower resistance are associated with better kidney function after transplantation.
Their research was funded by a grant from the Roche Organ Transplant Research Foundation and recently published in Annals of Surgery.
The United States has one of the world’s highest incidences of end-stage renal disease, and the number of afflicted individuals continues to increase. The prevalence of end-stage renal disease has more than doubled between 1990 and 2016, according to the Centers for Disease Control.
The optimal treatment is a kidney transplant, but demand far exceeds supply. Additionally, donation rates for deceased donors have been static for several years, despite various public-education campaigns, resulting in fewer kidneys available for transplant. And while the proportion and number of living donors has increased, this latter group still only makes up a small percentage of recovered kidneys for transplant.
Increasing the number of kidneys available for transplant benefits patients by extending lifespans and/or enhancing quality of life as well as the potential for reducing medical costs (a transplant is cheaper than ongoing dialysis). To help improve outcomes for kidney transplant patients, the team explored ways to extend the viability of donated kidneys.
Improvements in surgical techniques and immunosuppression therapies have made kidney transplants a relatively common procedure. However, less attention has been paid to maintaining/improving kidney function during the kidney-transport phase.
“We addressed this latter point through developing enhanced preservation methods,” said senior author James Reynolds, professor of Anesthesiology and Perioperative Medicine at Case Western Reserve School of Medicine and a member of the Harrington Discovery Institute at UH.
For decades, procured kidneys were simply flushed with preservation solution and then transported in ice-filled coolers to the recipient’s hospital. But advances in pumping technology slowly changed the field toward active storage, the preferred method for conveying the organ from donor to recipient.
“However, while 85% of kidneys are now pumped, up to 20% of kidneys are determined to be unsuitable for transplant during the storage phase,” said Kenneth Chavin, professor of surgery at the School of Medicine, chief of hepatobiliary and transplant surgery and director of the UH Transplant Institute.
“For several years, our team has directed research efforts toward understanding and improving the body’s response to medical manipulation,” Reynolds said. “Organ-donor physiology and ‘transport status’ fit well within this metric. We identified a therapy that might improve kidney perfusion, a significant factor in predicting how the organ will perform post-transplant.”
Previous work by Reynolds and long-time collaborator Jonathan Stamler, the Robert S. and Sylvia K. Reitman Family Foundation Distinguished Chair in Cardiovascular Innovation and president of the Harrington Discovery Institute, determined that brain death significantly reduces SNOs, which impairs blood-flow and tissue-oxygenation to the kidneys and other commonly transplanted organs. The loss of SNOs is not corrected by current preservation fluids, so impaired flow through the kidneys continues during storage and transport.
t’s been over a decade since artificial retinas first began helping the blind see. But for many people, whose blindness originates beyond the retina, the technology falls short. Which is why new research out of Spain skips the eye entirely, instead sending signals straight to the brain’s visual cortex.
Amazingly, 15 years after losing her sight, Bernardeta Gómez, who suffers from toxic optic neuropathy, used the experimental technology to recognize lights, letters, shapes, people—and even to play a basic video game sent directly to her brain via an implant.
According to MIT Technology Review, Gómez first began working with researchers in late 2018. Over the next six months, she spent four days a week dialing in the technology’s settings and testing its limits.
The system, developed by Eduardo Fernandez, director of neuroengineering at the University of Miguel Hernandez, works like this.
A camera embedded in a pair of thick, black-rimmed glasses records Gómez’s field of view and sends it to a computer. The computer translates the data into electrical impulses the brain can read and forwards it to a brain implant by way of a cable plugged into a port in the skull. The implant stimulates neurons in Gómez’s visual cortex, which her brain interprets as incoming sensory information. Gómez perceives a low-resolution depiction of her surroundings in the form of yellow dots and shapes called phosphenes which she’s learned to interpret as objects in the world around her.
The technology itself is still very much in the early stages—Gómez is the first to test it—but the team aims to work with five more patients in the next few years. Eventually, Fernandez hopes their efforts can help return sight to many more of the world’s blind people.
A Brief History of Artificial Eyes
This isn’t the first time researchers have used technology to help the blind see again.
Roughly two decades ago, the Artificial Retina Project brought together a number of research institutions to develop a device for those suffering retina-destroying diseases. The work resulted in the Argus systems, which, like Fernandez’s system, use a camera mounted on glasses, a computer to translate sensory data, and an implant with an array of electrodes embedded in the retina (instead of the brain).
Over the course of about a decade, researchers developed the Argus I and Argus II systems, ran them through human trials, and gained approval in Europe (2011) and the US (2013) to sell their bionic eyes to eligible individuals.
According to MIT Technology Review, around 350 people use Argus II today, but the company marketing the devices, Second Sight, has pivoted from artificial retinas to the brain itself because far more people, like Gómez, suffer from damage to the neural pathways between eyes and brain.
Just last year, Second Sight was involved in research, along with UCLA and Baylor, testing a system that also skips the retina and sends visual information straight to the brain.
The system, called Orion, is similar to Argus II. A feed from a video camera mounted on dark glasses is converted to electric pulses sent to an implant that stimulates the brain. The device is wireless and includes a belt with a button to amplify dark objects in the sun or light objects in the dark. Like Fernandez’s system, the user sees a low-resolution pattern of phosphenes they interpret as objects.
“I’ll see little white dots on a black background, like looking up at the stars at night,” said Jason Esterhuizen, who was the second research subject to receive the device. “As a person walks toward me, I might see three little dots. As they move closer to me, more and more dots light up.”
Though the research is promising—it’s designated an FDA Breakthrough Device and is being trialed with six patients—Dr. Daniel Yoshor, study leader and neurosurgeon, cautioned the Guardian last year that it’s “still a long way from what we hope to achieve.”
The Road Ahead
Brain implants are far riskier than eye implants, and if the original Argus system is any indication, it may be years before these new devices are used widely beyond research.
Still, brain-machine interfaces (BMIs) are quickly advancing on a number of fronts.
The implant used in Fernandez’s research is a fairly common device called a Utah array. The square array is a few millimeters wide and contains 100 electrode spikes which are inserted into the brain. Each spike stimulates a few neurons. Similar implants have helped paralyzed folks control robotic arms and type messages with just their thoughts.
Though they’ve been the source of several BMI breakthroughs, the arrays aren’t perfect.
The electrodes damage surrounding brain tissue, scarring renders them useless all too quickly, and they only interact with a handful of neurons. The ideal device would be wireless, last decades in the brain—limiting the number of surgeries needed—and offer greater precision and resolution.
Ferndandez believes his implant can be modified to last decades, and while the current maximum resolution is 10 by 10 pixels, he envisions one day implanting as many as 6 on each side of the brain to deliver a resolution of at least 60 by 60 pixels
In addition, new technologies are in the works. Famously, Elon Musk’s company Neuralink is developing soft, thread-like electrodes that are deftly laced into brain tissue by a robot. Neuralink is aiming to include 3,000 electrodes on their device to chat up far more neurons than is currently possible (though it’s not clear whether there’s a limit to how many more neurons actually add value). Still other approaches, that are likely further out, do away with electrodes altogether, using light or chemicals to control gene-edited neurons.
Fernandez’s process also relies on more than just the hardware. The team used machine learning, for example, to write the software that translates visual information into neural code. This can be further refined, and in the coming years, as they work on the system as a whole, the components will no doubt improve in parallel.
But how quickly it all comes together in a product for wider use isn’t clear.
Fernandez is quick to dial back expectations—pointing out that these are still early experiments, and he doesn’t want to get anyone’s hopes up. Still, given the choice, Gómez said she’d have elected to keep the implant and wouldn’t think twice about installing version two.
“This is an exciting time in neuroscience and neurotechnology, and I feel that within my lifetime we can restore functional sight to the blind,” Yoshor said last year.
Dr. Peter Pronovost: “So much of this work that I’m doing now is relational. It’s about building trusting relationships, because change progresses at the speed of trust, and trust grows when we do things with rather than to people.” (Gus Chan, The Plain Dealer)The Plain Dealer
By Brian Albrecht, The Plain Dealer
CLEVELAND, Ohio — The ghosts of medical errors haunt Dr. Peter Pronovost.
Two deaths, both caused by mistakes. First, his father’s, who died as the result of a cancer misdiagnosis. Then a little girl, a burn victim who succumbed to infection and diagnostic missteps at the hospital where Pronovost worked early in his career.
Those deaths led Pronovost to pursue a medical career dedicated to patient safety, and to create the medical checklist he has become known for worldwide.
Now, he’s implementing his second act, at University Hospitals, as its chief transformation officer, a job he has held since late 2018. His goal: To transform a $4 billion health care system by reducing shortcomings in medical care and increasing the quality of treatment.
The challenge fits Pronovost, says one of his former Johns Hopkins University professors, Dr. Albert Wu. “He’s one of the few people for whom the title might be appropriate, because his work has led to significant changes and innovations in how we deliver health care in the United States.
“He’s a once-in-a-generation guy.”
“One of the lasting impacts of the work we did in infections [with the checklist] was to change the belief that harm was inevitable,” says Dr. Peter Pronovost, chief transformation officer for University Hospitals. (Gus Chan, The Plain Dealer )The Plain Dealer
Taking the harm out of health care
Pronovost appears younger than his 54 years; he’s a self-described wellness fanatic, who loves running, biking, hiking and lifting weights. He’s comfortable at the office in everything from a pink, French cuff, button-down to an open-collar, checkered shirt.
In conversation, he can link medicine with a seemingly disparate array of subjects: United Kingdom economics, the shared learning of birds, the autobiographical nature of a Picasso painting. And yet, somehow, it all makes sense.
People who know him use words like charismatic, passionate, gifted, caring and high-energy to describe a physician whose prescription for health care reform combines research, bottom-line statistics and an unabashedly fervent dose of love.
Pronovost earned the nickname Dr. Checklist for his pioneering work 19 years ago developing a simple set of mandatory steps to eliminate infections from catheter lines, which once killed from 30,000 to 60,000 patients in the U.S. every year.
He wasn’t the first to use a checklist in medicine. But he’s been recognized as being among the first to maximize its use to save lives.
The success of the checklist concept spread to other medical procedures and has since become an accepted standard of health care and patient safety.
“We’ve shown with the checklist that we can take one problem and reduce it by 90 percent across the country,” Pronovost says. “What I want to do is broaden that and say, ‘Could I now take one health care system and eliminate defects in value . . . so we make health care much less harmful, much more affordable and more patient-centered?’
“But just like we did in my prior role, I want to create a model at UH and share it with the world.”
And checklists are very much involved in his vision.
Genesis of the checklist
Preparation for Pronovost’s life’s mission began when he was growing up in Waterbury, Conn. He credits his parents, an elementary school teacher and a mathematics professor, with providing needed support and validation of his views.
Pronovost says his high school study of philosophers like Plato and Socrates inspired an interest in understanding systems.
“One of the things I enjoy is stepping back and saying, ‘OK, here’s all the levers, here’s how the system works. How do we begin to pull those levers to move the needle in a big way?’ ” he says.
Thinking bigger led to the creation of his first checklist, one that tackles infections resulting from central line catheterization.
The process worked, spectacularly, and hospitals in other states and abroad started using the checklist model, which was gradually applied to other hospital procedures.
One application of the checklist concept was developed for blood clot prevention by Dr. Elliott R. Haut, vice chair of quality, safety and service at Johns Hopkins’ department of surgery.
Haut describes Pronovost as “super energetic. He’s a big thinker . . . a broad, how-to-change-the-world kind of guy.”
Pronovost will quickly point out that checklists alone “aren’t Harry Potter’s wand.”
They have to be part of a broader program that includes setting goals, building an enabling infrastructure, engaging with frontline clinicians and creating accountability systems.
When the checklist team started in 2001, at Johns Hopkins in Baltimore, an emphasis on patient safety in medical training and treatment was just in its infancy, You couldn’t even mention “human error” in a medical setting, says Bryan Sexton, now an associate professor of psychiatry and behavioral science at Duke University, who worked with Pronovost.
“Then, here comes this guy who looks like a Ken doll, out of nowhere. He brought science to the table and made it easy to do the right thing,” Sexton says.
“Peter Pronovost provided almost like a list of to-dos to get where [patient safety] needed to go. He was the right person at right time for something that was sorely needed.”
Accolades and accountability
In the years after the checklist debut, Pronovost gathered an array of accolades as he continued working in patient safety.
Time Magazine named Pronovost one of the 100 Most Influential People in the World in 2008, and that same year he won a MacArthur Foundation “genius” grant.
In 2003 he established the Quality and Safety Research Group at Johns Hopkins, and later became head of its Armstrong Institute for Patient Safety and Quality.
“Peter was very effective in positioning his center [the Armstrong Institute] as being about innovation and research, but sufficiently connected to the [health care] delivery system to make the changes that are necessary. His center really got it right,” says Dr. Bob Wachter, a patient safety expert and professor and chairman of the Department of Medicine at the University of California, San Francisco.
“I consider him to be one of the most important forces of my generation in health care,” says Dr. Thomas Lee, chief medical officer for Press Ganey, a national health-care consulting service. “Getting people to use the checklist took a special mix of confidence and passion and resilience. He earned the reputation he has for being a real leader.”
Pronovost helped The Leapfrog Group, a national organization that monitors hospital performance and encourages patient safety, develop its Hospital Safety Grade and annual Leapfrog Hospital Survey programs, says Leah Binder, president and CEO.
“We track reductions in deaths, errors and accidents, and I can say that through Leapfrog, he has saved thousands of lives,” Binder says. “He holds health care accountable for its performance.”
Beyond the checklists
There’s another side to Pronovost, says his daughter Emma.
“A lot of people only see the professional side of him. I get to see the fun side. He teaches me lot about not taking life too seriously,” says Emma, 19, a sophomore at Tulane University.
Like during one of the family’s ski trips when her father, knowing her fondness for dance, started singing waltzes, skiing to the beat, as they sped downhill together, to make her laugh.
And no, he doesn’t make checklists at home. Emma says that falls to her mother, Dr. Marlene R. Miller, pediatrician-in-chief for University Hospitals and chair of the Department of Pediatrics at Rainbow Babies & Children’s Hospital.
Driven and dedicated are words Ethan Pronovost, 22, a software engineer in San Francisco, uses to describe his father.
The dedication extends beyond working hours. Ethan says his father is constantly “looking for opportunities to expand his horizons.”
At work, “he really enjoys the propagation effect. It’s not just him, directly doing it himself, but inspiring others, building this cohort of influence.”
Pronovost’s wife of nearly 24 years is also a quality and safety researcher and says her husband’s qualities as a researcher include being “methodical, persistent. He brings good ideas to the table and then helps, through good analytical approaches, to make sure we can actually know if that intervention makes a difference.”
When asked how he’ll meet his newest challenge at University Hospitals, she laughs and says, “He’s been pretty successful so far. I don’t see that changing.”
Transforming a system
Pronovost cited a quote by poet Emily Dickinson, “Hope inspires the good to reveal itself,” to open a recent meeting of the team of health care specialists who are helping him transform University Hospitals.
He used the quote to illustrate a story about a homeless woman who repeatedly came to a UH hospital emergency room to ask for food. Instead of turning her away, the hospital arranged to have social services bring food to her home and helped resolve her other problems.
“In so much of health care we live these extremes of humanity where we can see what could be despair and self-destruction, or you can see hope and beauty and love,” Pronovost said. “All of us have that choice every day . . . whether we go to the dark and see the despair, or whether we have the hope and see the dignity.”
That said, the meeting got down to the business of the job he was hired for.
Pronovost and UH CEO Thomas Zenty co-developed several goals for the hospital system after Zenty hired the doctor in late 2018.
Their objectives capitalized on trends and challenges in health care, including:
Treat more people on an outpatient basis.
Utilize new technology that enables an increasing number of patients to be cared for at home.
Enhance the value of treatment and services to be more cost-effective and quality conscious.
Pronovost brought several attributes to the job, Zenty says. “Peter is not just a theoretician, but he is also very practical in terms of finding better ways to care for the patients we treat.”
He also was impressed by Pronovost’s work as a practicing physician, which enhances his credibility among fellow doctors, Zenty says.
Pronovost says the first challenge to providing the highest-value health care was identifying defects and working with others to eliminate them.
“We want to develop a new attitude that defects aren’t inevitable, but preventable, and value is all our responsibility,” he says.
Instead of the past “whack-a-mole” approach of trying to resolve individual health care problems as they surface, Pronovost says they organized their goals into three general areas:
Addressing patients’ needs for regular doctor visits, getting needed immunizations and screenings, and developing healthy habits.
Helping people with chronic diseases get well by reducing the risk of misdiagnosis and needless hospitalization.
Improving acute-care management, such as coordinating hospital care with a patient’s primary physician, and reducing unnecessary procedures (as many as 30 percent aren’t needed, Pronovost says).
Weekly interdisciplinary team meetings were established to plan policies, programs and, yes, checklists.
“[Attendees] all have very specific goals on their checklists. [Such as] how are we implementing protocols to reduce the length of [patient] stay and complications? How do we put the right rules in place so people go home rather than to a [skilled nursing facility], and that they get personal care-physician follow-up?” he says.
Pronovost notes that as a result of new efforts “we had about 1,000 to 1,200 fewer people readmitted” to the University Hospitals system last year.
Pronovost also says: There was a 12% increase in patients returning home, vs. a skilled nursing facility, after hospitalization. Acute care costs decreased by 25%. And, personal care physician follow-ups for post-hospital treatment went from 2% to 69%.
In just over a year since he was hired, Pronovost says, “We’re maybe 15 to 20% deployed in building this web of eliminating all these defects.”
Moving ahead
Pronovost is currently involved in an industry/government one-year Quality Summit to determine how to streamline programs administered by the U.S. Department of Health and Human Services to deliver a value-based care model. These programs include health care offered through Medicare, Medicaid and Veteran’s Affairs.
Part of that effort includes looking at the more than 2,000 measures the federal government uses to track health care quality. Pronovost says there needs to be a balance between unnecessary measures and those lacking in certain areas.
Additionally, Pronovost says, improving value in patient care and reducing preventable harm, the third leading cause of death, can trim health care costs, which run an estimated $3.5 trillion annually.
Pronovost’s program of value improvement and defect reduction at UH will probably take another four years to fully deploy, “and no doubt it will continue to get better and improve over time,” he says.
The launch of the n-Lorem Foundation by Ionis Pharmaceuticals’ Executive Chairman Stan Crooke last week began to crystallize the drug development pathway for ultra-rare diseases, but it also brought to the forefront a question raised in recent years with the maturation of genomic screening and antisense oligonucleotide (ASO) therapies: how can patients with ultra-rare diseases afford n-of-one therapies? The n-Lorem Foundation intends to form the connective tissue between patients, researchers, facilities and regulators needed to supply individual patients with RNA therapies designed to treat their own ultra-rare disease — at no cost. The nonprofit launched with $1.5 million from Crooke and his wife Rosanne, a senior strategic advisor at Ionis; $1.5 million from Ionis; and $1 million from Biogen.
As the founder and former CEO of Ionis, Crooke is in the best possible position to drive this formidable enterprise. Ionis was created to capitalize on ASO technology across a host of diseases, particularly rare ones. The company’s Spinraza (nusinersen), which was the first drug approved for spinal muscular atrophy and is marketed by its neurology partner, Biogen, is held up as the antisense field’s most notable commercial success. But although Spinraza made $547 million in revenue in 3Q19, there has never been a market for therapies in ultra-rare diseases, which n-Lorem considers as conditions with only one to ten patients.
Crooke says the fear that an entrepreneur would seek to monetize the space was a motivator in creating n-Lorem. “There’s no way to do that without targeting these families for millions of dollars. Patients and parents are raising money for their loved ones as a way to acquire an experimental treatment ASO. Given the burden these families have, the last thing they should have to do is raise money for their treatment.” The n-Lorem charity will ensure the patients they help will get the ASOs for free.
The concern that ultra-rare diseases might be treatable in theory but unaffordable in practice left the realm of the theoretical in October, with the publication of a New England Journal of Medicine paper on a treatment created from scratch for a girl with Batten’s disease by researchers at Boston Children’s Hospital and elsewhere. The scientists demonstrated, for the first time, how a single group can use genomic screening to diagnose an ultra-rare disease, develop an ASO drug for an individual patient, and within a year conduct an n-of-1 study yielding positive results. The news stoked hope that therapies for patients with one-of-a-kind diseases were possible to deliver. Timothy Yu, who led the Boston Children’s team, says his results show that, if the right incentives exist, the science and the technology are robust enough to deliver therapies.
Yu thinks academics will play a key role in developing n-of-one therapies, although they aren’t positioned to scale up yet. “We took a swing at something out of our comfort zone,” he says. “We were very fortunate.” “We need more data” from a more diverse range of drugs, Yu says, and that will shape how the space grows. n-Lorem will likely encourage further therapeutic development and a better model will emerge. For instance, one model could resemble how surgery or transplants are delivered in accredited hospitals using predefined processes designed for high-risk interventions.
Yu’s group had worked with Ionis to design and develop the ASO drug tailored to treat that single patient with a rare, fatal neurodegenerative condition, Crooke says. Even before that work became public, planning for n-Lorem had begun in earnest. Crooke, who announced a year ago he was stepping down as Ionis CEO but remains its board chairman, recalls the key event for the creation of n-Lorem as his introduction to the Undiagnosed Diseases Network. The initiative, funded by the US National Institutes of Health (NIH), connects patients with ultra-rare diseases with a consortium of 17 academic medical centers that perform multi-omic screening to help diagnose and understand the diseases. The network has evaluated over 1,300 patients and over 360 have received a diagnosis. “There was a cadre of physicians, scientists and genomicists that was actually doing the front end [the diagnosis],” says Crooke. “The back end [producing the drug] I already knew because antisense technology at Ionis is extraordinarily efficient. We have multiple mechanisms we can use.”
The technology needed for oligonucleotide synthesis is decades old, and Yu says manufacturing a batch of research grade oligonucleotides costs in the hundreds of dollars.
But Crooke says that the kinds of facilities Ionis uses are well suited for large batches; they are not built to produce small quantities for individual patients. As a result, bringing down the cost of manufacturing at this scale will be a problem n-Lorem and Ionis will continue to grapple with.
Patients will connect to n-Lorem via academics working through the Undiagnosed Diseases Network and beyond. The foundation will identify eligible patients and Ionis will develop the ASOs, perform preclinical testing and submit Investigational New Drug (IND) applications along with investigators.
To formalize the ASO development process, Ionis will need buy-in from regulators. The usual safety studies will necessarily apply, and Arthur Krieg, a cofounder of the Oligonucleotide Therapeutics Society, says the largest cost in developing therapies is toxicology studies. “This is where it will be tough for FDA and academic medical centers: how far back can we safely cut? You don’t want to endanger patients.”
Given the frequently dire circumstances of ultra-rare disease patients, n-Lorem is counting on flexibility from the FDA when it comes to preclinical requirements, which would save both time and cost. But it is unclear what that flexibility would entail. Crooke’s early interactions with the FDA gave him a “general sense” that toxicology testing requirements would be manageable but expects it will be some time before he receives definitive answers from the agency.
In the Batten’s disease instance, Yu’s lab worked with TriLink and Brammer to manufacture milasen,and with Charles River Laboratories to develop the toxicology and dose-finding studies. FDA agreed to review safety and manufacturing data on a rolling basis, allowing the drug to reach the patient just six weeks after it was first introduced to the rat model. But it is unclear whether the process can be easily reproduced by researchers, or if the expedited review is scalable at FDA
Testing requirements for ultra-rare disease therapies like the ASOs pursued by n-Lorem will have implications beyond just a handful of patients. In an editorial accompanying Yu’s paper, Janet Woodcock, and Peter Marks from the FDA’s Center for Drug Evaluation and Research, wrote that “programs for a single patient are likely to set the floor for the minimum preclinical evaluation.” They added that although in the near term ultra-rare therapies could exist as investigational drugs only, regulatory approval would become more pertinent if similar interventions begin to proliferate.
Woodcock told Nature Biotechnology that the agency is planning to issue guidances but did not give a time frame for their release. She noted the FDA has seen an increase in applications for n-of-1 studies from academics. There are no plans to use phase 0 trials or accredit hospitals, she says, as hospital pharmacies are unlikely to have the technology required to support the therapies. For now, researchers will continue to file an IND application for first-in-human studies for each ultra-rare therapeutic, a process she said will likely be difficult to sustain for n-Lorem or academic medical centers. She hopes companies will try developing n-of-one therapies as a probe for their technology or a proof of concept, where a similar intervention is developed for a more common disease or mutation.
Krieg says members of the Oligonucleotide Therapeutics Society — which divide roughly 50–50 between industry and academic scientists — are increasingly setting up centers for oligonucleotide development. In fact, growing interest in ASO technology for use in the ultra-rare disease space led him to organize a workshop with non-commercial stakeholders, including the NIH and FDA, in April 2020 to discuss how to facilitate effective oligonucleotide drug development programs. Krieg would like to see the space opened up to treat as many patients who could benefit from ASO technology as possible, which he thinks will require the development of guidelines and protocols. If the regulatory process remains the same as it is for a traditional drug, says Krieg, “it would be slow and costly, and a ton of work for FDA” as they parse potentially hundreds if IND applications from patients seeking new therapies. “As with CAR-Ts [chimeric antigen receptor T cells] or personalized vaccines, we need a process,” he says, and he hopes to see comparable guidance from FDA this year on n-of-one therapeutics.
Another key challenge is how to connect patients with institutions making tailor-made oligos. The n-Lorem Foundation is a step in the right direction, says Krieg, but “I’m hearing other philanthropic sources ready to put millions in,” and charity may not by the only middle way between individual academics and market-driven approaches. The NIH could have a role bridging the gap, through an intramural center or ASO centers of excellence funded in the same way as its cancer ones delivering CAR-T therapies that are, in a sense, individual therapies.
Although Krieg doesn’t yet see opportunities for companies to go after therapies for “less than a thousand patients,” unlike Crooke he thinks market development could be a positive. Individualized CAR-T therapies like Novartis’s Kymriah (tisagenlecleucel) and Gilead’s Yescarta (axicabtagene ciloleucel) cost upwards of $370,000, and medical costs for the first patients with ultra-rare diseases receiving ASOs run above $1 million, but Krieg says this doesn’t have to be discouraging. “Why couldn’t we have ASO therapies like CAR-T cells that insurance companies pay for?” He added that n-of-1 therapies could still be less expensive than the alternative: a lifetime of care.
The FDA has approved Caplyta for the treatment of schizophrenia in adults, according to a press release from the agent’s manufacturer.
“We believe Caplyta provides health care providers a new, safe and effective treatment option to help the millions of adult patients with schizophrenia,” Sharon Mates, PhD, chairman and CEO of Intra-Cellular Therapies, said in the release. “This approval represents the culmination of years of scientific research. We are especially grateful to the patients, their caregivers and the health care professionals who have contributed to the development of Caplyta.”
Caplyta (lumateperone, Intra-Cellular Therapies Inc.) demonstrated efficacy in two placebo-controlled trials that showed a statistically significant separation from placebo on the Positive and Negative Syndrome Scale total score. In these trials, the most common adverse reactions for the recommended dose (42 mg) of Caplyta vs. placebo were somnolence/sedation (24% vs. 10%) and dry mouth (6% vs. 2%).
Pooled data from short-term studies revealed similar outcomes between Caplyta and placebo for fasting glucose, mean changes from baseline in weight gain, triglycerides and total cholesterol. Further, the incidence of extrapyramidal symptoms was 6.7% for Caplyta vs. 6.3% for placebo.
Although the mechanism of action for Caplyta is currently unknown, its efficacy may be mediated through a combination of antagonist activity at central serotonin 5-HT2A receptors and postsynaptic antagonist activity at central dopamine D2 receptors, according to the release. Intra-Cellular Therapies expects to initiate the commercial launch of Caplyta in the first quarter of 2020.
The drug is being further developed to treat disorders beyond schizophrenia, including bipolar depression, behavioral disturbances in patients with dementia, depression and other neurological and neuropsychiatric disorders.
“Schizophrenia is a complex disease that severely impacts patients and their families,” Jeffrey A. Lieberman, MD, Lawrence C. Kolb Professor and Chairman of psychiatry at Columbia University’s College of Physicians and Surgeons, said in the release. “Effective treatment provided in a timely fashion can be game-changing for people living with schizophrenia. The efficacy and safety profile of Caplyta approved by the FDA offers health care providers an important new option for treating people living with schizophrenia.”
Neurons in the brain. Rather than implanting directly into the brain, the bionic neurons are built into ultra-low power microchips that form the basis for devices that would plug straight into the nervous system.
Scientists have created artificial neurons that could potentially be implanted into patients to overcome paralysis, restore failing brain circuits, and even connect their minds to machines.
The bionic neurons can receive electrical signals from healthy nerve cells, and process them in a natural way, before sending fresh signals on to other neurons, or to muscles and organs elsewhere in the body.
One of the first applications may be a treatment for a form of heart failure that develops when a particular neural circuit at the base of the brain deteriorates through age or disease and fails to send the right signals to make the heart pump properly.
Rather than implanting directly into the brain, the artificial neurons are built into ultra-low power microchips a few millimetres wide. The chips form the basis for devices that would plug straight into the nervous system, for example by intercepting signals that pass between the brain and leg muscles.
“Any area where you have some degenerative disease, such as Alzheimer’s, or where the neurons stop firing properly because of age, disease, or injury, then in theory you could replace the faulty biocircuit with a synthetic circuit,” said Alain Nogaret, a physicist who led the project at the University of Bath.
The breakthrough came when researchers found they could model live neurons in a computer program and then recreate their firing patterns in silicon chips with more than 94% accuracy. The program allows the scientists to mimic the full variety of neurons found in the nervous system.
Writing in the journal Nature Communications, the researchers describe how they fed the program with data recorded from two types of rat neuron, which were stimulated in a dish. The neurons were either from the hippocampus, a region that is crucial for memory and learning, or were involved in the subconscious control of breathing.
Armed with the program, the researchers claim they can now build bionic neurons based on any of the real nerve cells found in the brain, spinal cord, or the more distant reaches of the peripheral nervous system, such as the sensory neurons in the skin.
Because the artificial neurons both receive and send signals, they can be used to make implants that respond to neural feedback signals that are constantly coursing around the body.
“The potential is endless in terms of understanding how the brain works, because we now have the fundamental understanding and insight into the functional unit of the brain, and indeed applications, which might be to improve memory, to overcome paralysis and ameliorate disease,” said Julian Paton, a co-author on the study who holds posts at the Universities of Bristol and Auckland.
“They can be used in isolation or connected together to form neuronal networks to perform brain functions,” he added.
With development, trials and regulations to satisfy, it could be many years before the artificial neurons are helping patients. But if they prove safe and effective, they could ultimately be used to circumvent nerve damage in broken spines and help paralysed people regain movement, or to connect people’s brains to robotic limbs that can send touch sensations back through the implant to the brain.
Despite the vast possibilities the artificial neurons open up, Nogaret said the team was nowhere near building a whole brain, an organ which in a human consists of 86bn neurons and at least as many supporting cells. “We are not claiming that we are building a brain, there’s absolutely no way,” he said.
The scientists’ approach differs from that taken by many other peers who hope to recreate brain activity in computers. Rather than focusing on individual neurons, they typically model brain regions or even whole brains, but with far less precision. For example, the million-processor SpiNNaker machine at the University of Manchester can model an entire mouse brain, but not to the level of individual brain cells.
“If you wanted to model a whole mouse brain using the approach in this paper you might end up designing 100 million individual, but very precise, neurons on silicon, which is clearly unfeasible within a reasonable time and budget,” said Stephen Furber, professor of computer engineering at the University of Manchester.
“Because the approach is detailed and laboriously painstaking, it can really only be applied in practice to smallish neural units, such as the respiratory neurons described above, but there are quite a few critical small neural control circuits that are vital to keeping us alive,” he added.
Case Western Reserve researchers use AI with routine CT scans to predict how well lung cancer patients will respond to expensive treatment based off changes in texture patterns inside and outside the tumor.
Scientists from the Case Western Reserve University digital imaging lab, already pioneering the use of artificial intelligence (AI) to predict whether chemotherapy will be successful, can now determine which lung-cancer patients will benefit from expensive immunotherapy.
And, once again, they’re doing it by teaching a computer to find previously unseen changes in patterns in CT scans taken when the lung cancer is first diagnosed compared to scans taken after the first two to three cycles of immunotherapy treatment. And, as with previous work, those changes have been discovered both inside—and outside—the tumor, a signature of the lab’s recent research.
“This is no flash in the pan—this research really seems to be reflecting something about the very biology of the disease, about which is the more aggressive phenotype, and that’s information oncologists do not currently have,” said Anant Madabhushi, whose Center for Computational Imaging and Personalized Diagnostics (CCIPD) has become a global leader in the detection, diagnosis and characterization of various cancers and other diseases by meshing medical imaging, machine learning and AI.
Currently, only about 20% of all cancer patients will actually benefit from immunotherapy, a treatment that differs from chemotherapy in that it uses drugs to help your immune system fight cancer, while chemotherapy uses drugs to directly kill cancer cells, according to the National Cancer Institute.
Madabhushi said the recent work by his lab would help oncologists know which patients would actually benefit from the therapy, and who would not.
“Even though immunotherapy has changed the entire ecosystem of cancer, it also remains extremely expensive—about $200,000 per patient, per year,” Madabhushi said. “That’s part of the financial toxicity that comes along with cancer and results in about 42% of all new diagnosed cancer patients losing their life savings within a year of diagnosis.”
Having a tool based on the research being done now by his lab would go a long way toward “doing a better job of matching up which patients will respond to immunotherapy instead of throwing $800,000 down the drain,” he added, referencing the four patients out of five who will not benefit, multiplied by annual estimated cost.
Case Western Reserve researchers use AI with routine CT scans to predict how well lung cancer patients will respond to expensive treatment based off changes in texture patterns inside and outside the tumor
Scientists from the Case Western Reserve University digital imaging lab, already pioneering the use of artificial intelligence (AI) to predict whether chemotherapy will be successful, can now determine which lung-cancer patients will benefit from expensive immunotherapy.
And, once again, they’re doing it by teaching a computer to find previously unseen changes in patterns in CT scans taken when the lung cancer is first diagnosed compared to scans taken after the first two to three cycles of immunotherapy treatment. And, as with previous work, those changes have been discovered both inside—and outside—the tumor, a signature of the lab’s recent research.
“This is no flash in the pan—this research really seems to be reflecting something about the very biology of the disease, about which is the more aggressive phenotype, and that’s information oncologists do not currently have,” said Anant Madabhushi, whose Center for Computational Imaging and Personalized Diagnostics (CCIPD) has become a global leader in the detection, diagnosis and characterization of various cancers and other diseases by meshing medical imaging, machine learning and AI.
Currently, only about 20% of all cancer patients will actually benefit from immunotherapy, a treatment that differs from chemotherapy in that it uses drugs to help your immune system fight cancer, while chemotherapy uses drugs to directly kill cancer cells, according to the National Cancer Institute.
Madabhushi said the recent work by his lab would help oncologists know which patients would actually benefit from the therapy, and who would not.
“Even though immunotherapy has changed the entire ecosystem of cancer, it also remains extremely expensive—about $200,000 per patient, per year,” Madabhushi said. “That’s part of the financial toxicity that comes along with cancer and results in about 42% of all new diagnosed cancer patients losing their life savings within a year of diagnosis.”
Having a tool based on the research being done now by his lab would go a long way toward “doing a better job of matching up which patients will respond to immunotherapy instead of throwing $800,000 down the drain,” he added, referencing the four patients out of five who will not benefit, multiplied by annual estimated cost.
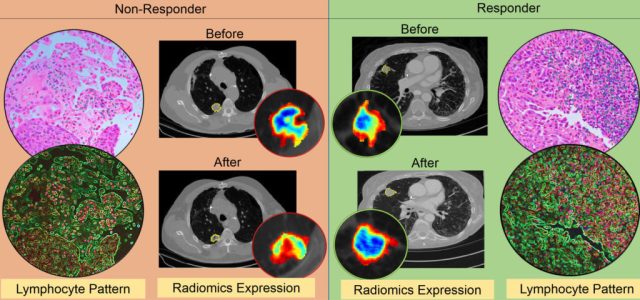
New research published The figure above shows differences in CT radiomic patterns before and after initiation of checkpoint inhibitor therapy.
The new research, led by co-authors Mohammadhadi Khorrami and Prateek Prasanna, along with Madabhushi and 10 other collaborators from six different institutions was published in November in the journal Cancer Immunology Research.
Khorrami, a graduate student working at the CCIPD, said one of the more significant advances in the research was the ability of the computer program to note the changes in texture, volume and shape of a given lesion, not just its size.
“This is important because when a doctor decides based on CT images alone whether a patient has responded to therapy, it is often based on the size of the lesion,” Khorrami said. “We have found that textural change is a better predictor of whether the therapy is working.
“Sometimes, for example, the nodule may appear larger after therapy because of another reason, say a broken vessel inside the tumor—but the therapy is actually working. Now, we have a way of knowing that.”
Prasanna, a postdoctoral research associate in Madabhushi’s lab, said the study also showed that the results were consistent across scans of patients treated at two different sites and with three different types of immunotherapy agents.
“This is a demonstration of the fundamental value of the program, that our machine-learning model could predict response in patients treated with different immune checkpoint inhibitors,” he said. “We are dealing with a fundamental biological principal.”
Prasanna said the initial study used CT scans from 50 patients to train the computer and create a mathematical algorithm to identify the changes in the lesion. He said the next step will be to test the program on cases obtained from other sites and across different immunotherapy agents. This research recently won an ASCO 2019 Conquer Cancer Foundation Merit Award.
Additionally, Madabhushi said, researchers were able show that the patterns on the CT scans which were most associated with a positive response to treatment and with overall patient survival were also later found to be closely associated with the arrangement of immune cells on the original diagnostic biopsies of those patients.
This suggests that those CT scans actually appear to capturing the immune response elicited by the tumors against the invasion of the cancer—and that the ones with the strongest immune response were showing the most significant textural change and most importantly, would best respond to the immunotherapy, he said.
Madabhushi established the CCIPD at Case Western Reserve in 2012. The lab now includes nearly 60 researchers.
Some of the lab’s most recent work, in collaboration with New York University and Yale University, has used AI to predict which lung cancer patients would benefit from adjuvant chemotherapy based on tissue-slide images. That advancement was named by Prevention Magazine as one of the top 10 medical breakthroughs of 2018.
Other authors on the paper were: Germán Corredor, Mehdi Alilou and Kaustav Bera from biomedical engineering, Case Western Reserve University; Pingfu Fu from population and quantitative health sciences, Case Western Reserve University; Amit Gupta of University Hospitals Cleveland Medical Center; Pradnya Patil of Cleveland Clinic; Priya D. Velu of Weill Cornell Medicine; Rajat Thawani of Maimonides Medical Center; Michael Feldman from Perelman School of Medicine of the University of Pennsylvania; and Vamsidhar Velcheti from NYU-Langone Medical Center.
For more information, contact Mike Scott at mike.scott@case.edu.
Doctors have placed humans in suspended animation for the first time, as part of a trial in the US that aims to make it possible to fix traumatic injuries that would otherwise cause death.
Samuel Tisherman, at the University of Maryland School of Medicine, told New Scientist that his team of medics had placed at least one patient in suspended animation, calling it “a little surreal” when they first did it. He wouldn’t reveal how many people had survived as a result.
The technique, officially called emergency preservation and resuscitation (EPR), is being carried out on people who arrive at the University of Maryland Medical Centre in Baltimore with an acute trauma – such as a gunshot or stab wound – and have had a cardiac arrest. Their heart will have stopped beating and they will have lost more than half their blood. There are only minutes to operate, with a less than 5 per cent chance that they would normally survive.
EPR involves rapidly cooling a person to around 10 to 15°C by replacing all of their blood with ice-cold saline. The patient’s brain activity almost completely stops. They are then disconnected from the cooling system and their body – which would otherwise be classified as dead – is moved to the operating theatre.
A surgical team then has 2 hours to fix the person’s injuries before they are warmed up and their heart restarted. Tisherman says he hopes to be able to announce the full results of the trial by the end of 2020.
At normal body temperature – about 37°C – our cells need a constant supply of oxygen to produce energy. When our heart stops beating, blood no longer carries oxygen to cells. Without oxygen, our brain can only survive for about 5 minutes before irreversible damage occurs. However, lowering the temperature of the body and brain slows or stops all the chemical reactions in our cells, which need less oxygen as a consequence.
Tisherman’s plan for the trial was that 10 people who receive EPR will be compared with 10 people who would have been eligible for the treatment but for the fact that the correct team wasn’t in the hospital at the time of admittance.
The trial was given the go-ahead by the US Food and Drug Administration. The FDA made it exempt from needing patient consent as the participants’ injuries are likely to be fatal and there is no alternative treatment. The team had discussions with the local community and placed ads in newspapers describing the trial, pointing people to a website where they can opt out.
Tisherman’s interest in trauma research was ignited by an early incident in his career in which a young man was stabbed in the heart after an altercation over bowling shoes. “He was a healthy young man just minutes before, then suddenly he was dead. We could have saved him if we’d had enough time,” he says. This led him to start investigating ways in which cooling might allow surgeons more time to do their job.
Animal studies showed that pigs with acute trauma could be cooled for 3 hours, stitched up and resuscitated. “We felt it was time to take it to our patients,” says Tisherman. “Now we are doing it and we are learning a lot as we move forward with the trial. Once we can prove it works here, we can expand the utility of this technique to help patients survive that otherwise would not.”
“I want to make clear that we’re not trying to send people off to Saturn,” he says. “We’re trying to buy ourselves more time to save lives.”
In fact, how long you can extend the time in which someone is in suspended animation isn’t clear. When a person’s cells are warmed up, they can experience reperfusion injuries, in which a series of chemical reactions damage the cell – and the longer they are without oxygen, the more damage occurs.
It may be possible to give people a cocktail of drugs to help minimise these injuries and extend the time in which they are suspended, says Tisherman, “but we haven’t identified all the causes of reperfusion injuries yet”.
Tisherman described the team’s progress on Monday at a symposium at the New York Academy of Sciences. Ariane Lewis, director of the division of neuro-critical care at NYU Langone Health, said she thought it was important work, but that it was just first steps. “We have to see whether it works and then we can start to think about how and where we can use it.”
At one point, Zach Wigal had 5,000 video games in his parents’ basement.
Yes, 5,000. But it’s not what you might think.
Wigal is the founder of Gamers Outreach, a nonprofit that makes sure that kids who can’t leave their hospital rooms during long-term medical treatment can play video games while they recuperate.
“We noticed that a lot of the video games (at the hospitals) were getting stuck in playrooms,” said Wigal, 29. “And because of that, there was a whole segment of the hospital population that was, sort of, limited to whatever it was they had access to their bedside environment.”
Those 5,000 games eventually made their way out of his parents’ basement and some were featured on simple, portable video game carts that Wigal’s foundation helped design and provide to more than a million kids a year.
These “GOKarts” — equipped with a gaming console and an array of video games — are rolled into a patient’s room and allow kids “a source of fun and relief during … stressful and difficult times,” Wigal said.
Some kids have seen health benefits as a result, and doctors are prescribing “video game time” for certain patients, according to Andrew Gabanyicz, patient technologist at C.S. Mott Children’s Hospital in Ann Arbor, Michigan.
“We’ve seen anxiety go down, prescription pain killers are being used less,” Gabanyicz said.
Wigal’s inspiration for his charity came from his love of gaming as a teen — which took an interesting turn during his junior year of high school.
He registered more than 300 fellow students to participate in a Halo 2 tournament in his high school cafeteria. He rented the space with permission from the school. He spent months organizing it.
Then BAM.
“This event got shut down a couple days before it was supposed to happen by a police officer who believed that games like Halo were, in his words, corrupting the minds of America’s youth,” Wigal said. “Everyone who had signed up for our video game tournament was a little upset.”
The cancellation sparked an idea: Wigal wanted to show authorities that gamers weren’t all bad or lazy kids — and they could do something good with their gaming skills.
So he decided to throw a new tournament. The twist: He would donate the proceeds to charity. In 2008, Wigal and his friends held an event called Gamers for Giving and raised money for the Autism Society of America.
“I thought, ‘Let’s illustrate the positive things that can happen when gamers get together around what they’re passionate about,'” said Wigal, once named to Forbes Magazine’s 30 under 30.
The event continued year after year, and as it grew in popularity, Wigal’s team branched out and started working with local hospitals. In 2009, Wigal began working with the C.S. Mott Children’s Hospital and his team designed his portable GOKarts.
“We work with kids that can’t go on the soccer field. They physically cannot participate. But I don’t feel like they should be missing out on the values that are communicated through traditional activities,” Wigal said.
CNN’s Allie Torgan spoke with Wigal about his work. Below is an edited version of their conversation.
CNN: As a teenager, your parents’ house was ground zero for charitable operations. What was the straw that broke the camel’s back, so to speak?
Zach Wigal: We had taken over my parents’ basement raising money for Gamers Outreach. It had become this holding area for gaming equipment that was being donated to our organization for use in the hospital environment. There was a period of time we had, I kid you not, more than 5,000 video games in my parents’ basement.
We actually had someone donate, like, 900 Xboxes that had just been sitting in a warehouse. Thankfully my parents just had the patience to be okay with all of this up until that semi-truck wanted to show up, and that was the day it was like, “It’s not going to go in the basement. You need to find a place for all this equipment.” That was the day we got kicked out of my parents’ house! Now we have a warehouse here in Michigan.
CNN: Your signature GOKarts are now serving more than a million kids a year at 50 hospitals. Why that model?
Wigal: By volunteering and visiting hospitals, we were noticing that it was difficult to bring technology into these environments. We noticed that a lot of the video games were getting stuck in playrooms. And because of that, there was a whole segment of the hospital population that was, sort of, limited to whatever it was they had access to their bedside environment if they couldn’t leave their rooms.
Sometimes you have families that can’t afford technology or they don’t have things that they can bring from home for their kids. It becomes important for technology and hardware to exist in the hospital environment to help provide some access to entertainment to patients who maybe can’t do things outside of their room.
CNN: What advice do you have for parents of patients who may be struggling with how much screen time is appropriate?
Wigal: Even if you’re not a fan of gaming or screen time or you feel it might be excessive, technology is a prevalent part of all our lives. I mean, even my mom has Angry Birds installed on her cell phone at this point.
What’s important is that we communicate the right values of how this technology plays a role in our life, how we balance technology with being healthy as an individual and taking care of your mental health, keeping up with schoolwork, finding a career. These are all things that can exist cohesively.
We think of the work we’re doing as an opportunity to improve a patient’s quality of life. We’re coming to provide entertainment into hospital environments. We’re helping kids to find a source of fun and relief during times where being in the hospital can be really stressful and difficult otherwise.
Want to get involved? Check out the Gamers Outreach website and see how to help.
High doses of vitamin D taken one hour after sunburn significantly reduce skin redness, swelling, and inflammation, according to double-blinded, placebo-controlled clinical trial out of Case Western Reserve University School of Medicine and University Hospitals Cleveland Medical Center. The trial results were recently published in the Journal of Investigative Dermatology.
In the study, 20 participants were randomized to receive a placebo pill or 50,000, 100,000, or 200,000 IU of vitamin D one hour after a small UV lamp “sunburn” on their inner arm. Researchers followed up with the participants 24, 48, 72 hours and 1 week after the experiment and collected skin biopsies for further testing. Participants who consumed the highest doses of vitamin D had long-lasting benefits — including less skin inflammation 48 hours after the burn. Participants with the highest blood levels of vitamin D also had less skin redness and a jump in gene activity related to skin barrier repair.
“We found benefits from vitamin D were dose-dependent,” said Kurt Lu, MD, senior author on the study and Assistant Professor of Dermatology at Case Western Reserve University School of Medicine and University Hospitals Cleveland Medical Center. “We hypothesize that vitamin D helps promote protective barriers in the skin by rapidly reducing inflammation. What we did not expect was that at a certain dose, vitamin D not only was capable of suppressing inflammation, it was also activating skin repair genes.”
The trial is the first to describe acute anti-inflammatory benefits from taking vitamin D. According to the authors, despite widespread attention given to vitamin D deficiency, “there is a lack of evidence demonstrating that intervention with vitamin D is capable of resolving acute inflammation.” By measuring gene activity in the biopsies, the researchers also uncovered a potential mechanism behind how vitamin D aids skin repair. The results suggest vitamin D increases skin levels of an anti-inflammatory enzyme, arginase-1. The enzyme enhances tissue repair after damage and helps activate other anti-inflammatory proteins.
The study may have people flocking to vitamin supplement aisles, but Lu stresses that the trial tested very high doses of vitamin D that far exceed daily allowances. The Food and Drug Administration’s recommended adult daily allowance for vitamin D is 400 IU. Said Lu, “I would not recommend at this moment that people start taking vitamin D after sunburn based on this study alone. But, the results are promising and worthy of further study.” Lu and colleagues are planning additional studies that could inform treatment plans for burn patients.