ndividuals with acne have a significantly increased risk for depression within the first 5 years after receiving an acne diagnosis, according to a recent study.
For their study, Dr Isabelle Vallerand, of the University of Calgary in Canada, and colleagues obtained and evaluated patient data from the 1986-2012 Health Improvement Network (THIN) in the United Kingdom.
Results of the analysis revealed that individuals with acne had a 63% higher risk for depression within 1 year after diagnosis compared with individuals without acne, thus indicating the importance of evaluating patients with acne for symptoms of depression.
“This study highlights an important link between skin disease and mental illness,” Dr Vallerand said in a press release.
“Given the risk of depression was highest in the period right after the first time a patient presented to a physician for acne concerns, it shows just how impactful our skin can be towards our overall mental health.”
—Christina Vogt
Reference:
Vallerand IA, Lewinson RT, Parsons LM, et al. Risk of depression among patients with acne in the U.K.: a population-based cohort study [published online February 7, 2018]. Brit J Dermatol. doi:10.1111/bjd.16099.
wearing is usually regarded as simply lazy language or an abusive lapse in civility. But as Emma Byrne shows in her book, Swearing Is Good for You: The Amazing Science of Bad Language, new research reveals that profanity has many positive virtues, from promoting trust and teamwork in the office to increasing our tolerance to pain.
When National Geographic caught up with Byrne at her home in London, she explained why humans aren’t the only primates that can curse and why, though women are swearing more today than before, it is still regarded by many as “unfeminine.”
You write, “I’ve had a certain pride in my knack for colorful and well-timed swearing.” Tell us about your relationship to bad language, and in what sense it is good for us?
My first memory of being punished for swearing was calling my little brother a four-letter word, twat, which I thought was just an odd pronunciation of the word twit. I must have been about eight at the time; my brother was still pre-school. My mother froze, then belted me round the ear. That made me realize that some words had considerably more power than others, and that the mere shift in a vowel was enough to completely change the emotional impact of a word.
I’ve always had a curiosity about things I’ve been told I am not meant to be interested in, which is why I wound up in a fairly male-dominated field of artificial intelligence for my career. There’s a certain cussedness to my personality that means, as soon as someone says, “No, that’s not for you,” I absolutely have to know about it.
My relationship with swearing is definitely one example. I tend to use it as a way of marking myself out as being more like my male colleagues, like having a working knowledge of the offside rule in soccer. It’s a good way of making sure that I’m not seen as this weird, other person, based on my gender.
There’s great research coming out of Australia and New Zealand, which is perhaps not surprising, that says that jocular abuse, particularly swearing among friends, is a strong signal of the degree of trust that those friends share. When you look at the transcripts of these case studies of effective teams in sectors like manufacturing and IT, those that can joke with each other in ways that transgress polite speech, which includes a lot of swearing, tend to report that they trust each other more.
One of the reasons why there’s probably this strong correlation is that swearing has such an emotional impact. You’re demonstrating that you have a sophisticated theory of mind about the person that you’re talking to, and that you have worked out where the limit is between being shocking enough to make them giggle or notice you’ve used it but not so shocking that they’ll be mortally offended. That’s a hard target to hit right in the bullseye. Using swear words appropriate for that person shows how well you know them; and how well you understand their mental model.
You were inspired to write this book by a study carried out by Dr. Richard Stephens. Tell us about the experiment, and why it was important in our understanding of swearing.
Richard Stephens works out of Keele University in the U.K. He’s a behavioral psychologist, who is interested in why we do things that we’ve been told are bad for us. For years, the medical profession has been saying that swearing is incredibly bad for you if you’re in pain. It’s what’s called a “catastrophizing response,” focusing on the negative thing that’s happened. His take on this was, if it’s so maladaptive, why do we keep doing it?
He initially had 67 volunteers, although he’s replicated this multiple times. He stuck their hands in ice water and randomized whether or not they were using a swear word or a neutral word and compared how long they could keep their hands in ice water. On average, when they were swearing they could keep their hands in the iced water for half as long again as when they were using a neutral word. This shows that the results are anything but maladaptive. Swearing really does allow you to withstand pain for longer.
Have men always sworn more than women? And, if so, why?
Definitely not! Historians of the English language describe how women were equally praised for their command of exceedingly expressive insults and swearing, right up to the point in 1673 when a book by Richard Allestree was published titled The Ladies Calling.” Allestree says that women who swear are acting in a way that is biologically incompatible with being a woman and, as a result, will begin to take on masculine characteristics, like growing facial hair or becoming infertile. He wrote, “There is no sound more odious to the ears of God than an oath in the mouth of a woman.”
Today we are horribly still in the same place on men versus women swearing. Although women are still considered to swear less than men, we know from studies that they don’t. They swear just as much as men. But attitudinal surveys show that both men and women tend to judge women’s swearing much more harshly. And that judgement can have serious implications. For example, when women with breast cancer or arthritis swear as a result of their condition, they’re much more likely to lose friends, particularly female friends. Whereas men who swear about conditions like testicular cancer tend to bond more closely with other men using the same vocabulary. The idea that swearing is a legitimate means of expressing a negative emotion is much more circumscribed for women.
I was fascinated to discover that it’s not just humans that swear—primates do it, too! Tell us about Project Washoe.
Out in the wild, chimps are inveterate users of their excrement to mark their territory or show their annoyance. So the first thing you do, if you want to teach a primate sign language, is potty train them. That means, just like human children at a similar age, that they end up with a taboo around excrement. In Project Washoe, the sign for “dirty” was bringing the knuckles up to the underside of the chin. And what happened spontaneously, without the scientists teaching them, was that the chimps started to use the sign for “dirty” in exactly the same way as we use our own excremental swear words.
Washoe was a female chimpanzee that was originally adopted by R. Allen Gardner and Beatrix T. Gardner in the 1960s. Later, she was taken on by a researcher in Washington State called Roger Fouts. Washoe was the matriarch to three younger chimps: Loulis, Tatu, and Dar. By the time they brought in Loulis, the youngest, the humans had stopped teaching them language, so they looked to see if the chimps would transmit language through the generations, which they did.
Not only that: as soon as they had internalized the toilet taboo, with the sign “dirty” as something shameful, they started using that sign as an admonition or to express anger, like a swear word. When Washoe and the other chimps were really angry, they would smack their knuckles on the underside of their chins, so you could hear this chimp-teeth-clacking sound.
Washoe and the other chimps would sign things like “Dirty Roger!” or “Dirty Monkey!” when they were angry. The humans hadn’t taught them this! What had happened is that they had internalized that taboo, they had a sign associated with that taboo, so all of a sudden that language was incredibly powerful and was being thrown about, just like real excrement is thrown about by wild chimpanzees.
You say, “swearing is a bellwether—a foul-beaked canary in the coalmine—that tells us what our social taboos are.” Unpack that idea for us, and how it has changed over the centuries.
The example that most people will be familiar with in English-speaking countries is blasphemy. There are still parts of the U.S. that are more observant of Christianity than others but, in general, the kinds of language that would have resulted in censorship in other eras is now freely used in print and TV media. However, the “n-word,” which was once used as the title of an Agatha Christie book and even in nursery rhymes, is now taboo because there is a greater awareness that it is a painful reminder of how African-Americans suffered because of racism over the centuries. In some communities, where that usage is reclaimed, they are saying that if I use it, it immunizes me against its negative effects.
That is an example of a word that has fallen out of general conversation and literature into the realm of the unsayable. It’s quite different from the copulatory or excretory swearing in that it is so divisive. The great thing about the copulatory and excretory swearing is that they are common to the entire human race.
In the digital world, you can swear at someone without actually being face to face. Is this changing the way we curse? And what will swearing in tomorrow’s world look like?
One of the difficulties with swearing in online discourse is that there is no face-to-face repercussion, so it allows people to lash out without seeing the person that they’re speaking to as fully human. But it’s not swearing that is the problem. It’s possible to say someone is worth less as a human being based on their race, gender or sexuality using the most civil of language. For example, when Donald Trump called Hillary Clinton “a nasty woman” rather than using the c-word, most of us were able to break the code. We knew what he meant but because he hadn’t sworn it was seen as acceptable discourse.
In the future, I think that swearing will inevitably be reinvented; we’ve seen it change so much over the years. As our taboos change, that core of language that has the ability to surprise, shock or stun the emotional side of the brain will change, too. But I can’t predict where those taboos will go.
lzheimer’s disease is a neurodegenerative condition that causes the decline of cognitive function and the inability to carry out daily life activities. Past studies have suggested depression and other neuropsychiatric symptoms may be predictors of AD’s progression during its “preclinical” phase, during which time brain deposits of fibrillar amyloid and pathological tau accumulate in a patient’s brain. This phase can occur more than a decade before a patient’s onset of mild cognitive impairment. Investigators at Brigham and Women’s Hospital examined the association of brain amyloid beta and longitudinal measures of depression and depressive symptoms in cognitively normal, older adults. Their findings, published today by The American Journal of Psychiatry, suggest that higher levels of amyloid beta may be associated with increasing symptoms of anxiety in these individuals. These results support the theory that neuropsychiatric symptoms could be an early indicator of AD.
“Rather than just looking at depression as a total score, we looked at specific symptoms such as anxiety. When compared to other symptoms of depression such as sadness or loss of interest, anxiety symptoms increased over time in those with higher amyloid beta levels in the brain,” said first author Nancy Donovan, MD, a geriatric psychiatrist at Brigham and Women’s Hospital. “This suggests that anxiety symptoms could be a manifestation of Alzheimer’s disease prior to the onset of cognitive impairment. If further research substantiates anxiety as an early indicator, it would be important for not only identifying people early on with the disease, but also, treating it and potentially slowing or preventing the disease process early on.” As anxiety is common in older people, rising anxiety symptoms may prove to be most useful as a risk marker in older adults with other genetic, biological or clinical indicators of high AD risk.
Researchers derived data from the Harvard Aging Brain Study, an observational study of older adult volunteers aimed at defining neurobiological and clinical changes in early Alzheimer’s disease. The participants included 270 community dwelling, cognitively normal men and women, between 62 and 90 years old, with no active psychiatric disorders. Individuals also underwent baseline imaging scans commonly used in studies of Alzheimer’s disease, and annual assessments with the 30-item Geriatric Depression Scale (GDS), an assessment used to detect depression in older adults.
The team calculated total GDS scores as well as scores for three clusters symptoms of depression: apathy-anhedonia, dysphoria, and anxiety. These scores were looked at over a span of five years.
From their research, the team found that higher brain amyloid beta burden was associated with increasing anxiety symptoms over time in cognitively normal older adults. The results suggest that worsening anxious-depressive symptoms may be an early predictor of elevated amyloid beta levels – and, in turn AD — and provide support for the hypothesis that emerging neuropsychiatric symptoms represent an early manifestation of preclinical Alzheimer’s disease.
Donovan notes further longitudinal follow-up is needed to determine whether these escalating depressive symptoms give rise to clinical depression and dementia stages of Alzheimer’s disease over time.
Paper cited: Donovan et al. “Longitudinal Association of Amyloid Beta and Anxious-Depressive Symptoms in Cognitively Normal Older Adults” The American Journal of Psychiatry DOI: 10.1176/appi.ajp.2017.17040442
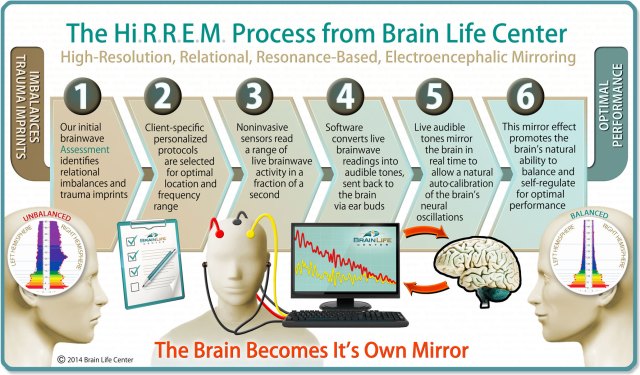
A noninvasive intervention that uses brainwave mirroring technology improved symptoms of post-traumatic stress, insomnia, anxiety and depressive mood for up to 6 months in service members and veterans, according to pilot study findings published in Military Medical Research.
“Ongoing symptoms of post-traumatic stress, whether clinically diagnosed or not, are a pervasive problem in the military,” Charles H. Tegeler, MD, professor of neurology at Wake Forest School of Medicine, said in a press release. “Medications are often used to help control specific symptoms, but can produce side effects. Other treatments may not be well tolerated, and few show a benefit for the associated sleep disturbance. Additional noninvasive, nondrug therapies are needed.”
In this study, researchers used high-resolution, relational, resonance-based, electroencephalic mirroring (HIRREM), a noninvasive neurotechnology that translates dominant brain frequencies into audible tones to support the auto-calibration of neural oscillations in real time. They collected data on symptoms of post-traumatic stress (PTS), insomnia, depression and anxiety from 18 military personnel with military-related PTS who received an average of 19.5 HIRREM sessions over 12 days. Researchers conducted follow-up online interviews at 1-, 3- and 6-months.
Tegeler and colleagues observed clinically significant reductions in all symptom scores immediately after intervention completion, with durability through 6 months. Through the first two follow-up visits, 83% of participants reported PTS scores that were at least 10 points lower than baseline and 78% reported insomnia scores that were at least seven points lower than baseline. For 15 participants with a history of traumatic brain injury or concussion, there were durable reductions in concussion-related symptoms. Additionally, participants also experienced significant improvements in blood pressure measures such as heart rate variability and baroreflex sensitivity. No adverse events were reported.
“We observed reductions in post-traumatic symptoms, including insomnia, depressive mood and anxiety that were durable through 6 months after the use of HIRREM, but additional research is needed to confirm these initial findings,” Tegeler said in the release. “This study is also the first to report improvement in heart rate variability and baroreflex sensitivity — physiological responses to stress — after the use of an intervention for service members or veterans with ongoing symptoms of post-traumatic stress.” – by Savannah Demko
Over the years, there’s been no shortage of interesting alternatives to typical talk-based psychotherapy. Laughter therapy, sound therapy, horticultural therapy and even wilderness therapy have become popular ways to deal with psychological distress, helping with everything from general anxiety and depression to post traumatic stress disorder (PTSD). These aren’t the only fascinating alternatives, though.
Another form of therapy is Eye Movement Desensitization and Reprocessing (EMDR), which can be an effective method for treating PTSD.
EMDR helps victims of trauma re-process and learn to cope with difficult events by rapidly moving their eyes back and forth, following the movement of a therapist’s finger while concentrating on a distressing memory.
The origins of EMDR
EMDR began practically by accident in 1987, when California psychologist Francine Shapiro was taking a walk in the woods, reports Scientific American.
During her stroll, Shapiro said she was anxious. She soon realized, though, that her anxiety had subsided once she began moving her eyes back and forth while at the same time closely observing and concentrating on her surroundings. Once she discovered that the rapid movement of her eyes brought her to a more relaxed state, she decided to see if rapid eye movement might reduce stress and anxiety in her clients. After finding that the procedure was able to help ease distress in her clients, Shapiro published a study in 1989 on her research, dubbing the practice EMDR.
Since then, EMDR has been used as a treatment for PTSD and various other conditions such as depression, schizophrenia, sexual dysfunction, stress and other anxiety disorders.
EMDR trainer Roger Solomon is a clinical psychologist whose specialty is trauma and grief. He is the police psychologist for the South Carolina Department of Public Safety and a consultant to the trauma programs of the U.S. Senate and several state and federal law enforcement agencies.
“EMDR therapy is guided by the Adaptive Information Processing model,” says Solomon. “This model posits that present problems are the result of past distressing memories that have become ‘frozen’ or stuck in the brain (including the images, thoughts and beliefs, feelings and sensations), thus becoming maladaptively stored in the brain. When there is a reminder (either external or internal), this maladaptively stored information gets triggered and is experienced in the present.”
Based on that premise, EMDR seeks to help people effectively adapt to their lives once trauma has occurred. EMDR gives those who suffer from trauma the possibility of reprocessing traumatic memories, so that the memories are able to become “unstuck” and processed in a way that the traumatized person is able to understand.
EMDR allows for what Solomon sees as the “the transmutation of the perpetual re-experiencing of distressing events with a learning experience that becomes a source of resilience.”
All this takes place by using a simple technique such as moving one’s eyes back and forth, which “stimulates the information processing mechanisms of the brain,” says Solomon. Once the information processing mechanism of the brain is stimulated by following the movements of the therapist’s fingers with the eyes, the traumatized person is able to reprocess the memories that cause distress; it gives them the ability to effectively adapt, learn and understand that he or she has successfully made it through the trauma.
AN EXAMPLE
To illustrate, Solomon uses the experience of a war veteran. “A war veteran experiencing a near-death experience in battle may have concluded ‘I am going to die,’ which becomes maladaptively stored in the brain, unable to process,” Solomon says. “When there is a present trigger, the distressing memory including the images, thoughts and beliefs and sensations associated with the event arise and are experienced as nightmares, flashbacks, and other symptoms of PTSD.”
Once the veteran is able to properly reprocess the information after undergoing EMDR, “the veteran can think of the battle event and know, at a felt body level, that ‘I survived, it’s over,’” says Solomon.
Theories behind the inner workings of reprocessing
Psychologists have come up with a number of theories as to how memory reprocessing during EMDR works — and more research is needed to determine the exact process — but here are a few that might explain exactly what’s happening in the brain during EMDR.
The working memory theory: Working memory is our short-term memory. It’s the part of our memory that allows us to store information that we need to reason, learn and comprehend.
“Studies looking at the specific effects of eye movements used in EMDR therapy show a significant reduction of memory vividness and associated emotion” says Solomon. “The working memory theory posits that the working memory system has a very limited capacity. When it is taxed by the competing tasks of holding a memory in mind while moving the eyes, there is a degradation of performance. This results in the distressing memory losing its quality and power.”
It’s almost as if the memory is unable to “keep up” with the reprocessing that occurs while the traumatized person’s eyes are moving back and forth — thus making the memory lose its grip over the person.
REM sleep theory: Rapid Eye Movement sleep (REM) is the stage of sleep in which we dream, and process and store memories.
Solomon explains that it’s “been hypothesized that eye movements stimulate the same neurological processes that take place during REM/dream sleep, which is important in processing and consolidating information.”
It’s possible the EMDR helps a person process a traumatic memory, in much the same way dreaming allows us to process the events of our daily lives while we sleep.
Memory reconsolidation theory: Memory reconsolidation is a process used by therapists to reorder and recode memories once a traumatic memory has been unlocked or accessed.
“Accessing a memory, and updating it with new contradictory information, enables the potential for the original memory to be transformed and reconsolidated, i.e., stored in altered form,” Solomon explains. “This differs from other trauma-focused therapies (e.g. Cognitive Behavioral Therapy) where the underlying mechanism is hypothesized to be habituation and extinction, which are thought to create a new memory, while leaving the original one intact.”
In this instance, the traumatic memory changes and transforms; it doesn’t disappear completely. Here, there aren’t two separate memories — one being the traumatic memory and the other being a memory which is of a peaceful nature. You have one memory which has transformed from trauma into a state of acceptance. This might explain the transmutation aspect of EMDR.
Parasympathetic nervous system theory: The parasympathetic nervous system is the part of our nervous system that helps us calm down and relax. It slows the heart, dilates blood vessels, relaxes the muscles in the gastrointestinal tract, increases digestive juices and decreases pupil size.
As far the relation between the parasympathetic nervous system and EMDR, Solomon says it’s possible that the “eye movements elicit an orienting response which activates the parasympathetic nervous system and lowers arousal.” Simply put, rapid eye movement and EMDR seem to be relaxing. “This theory has support from research showing that eye movement lowers arousal for distressing memories,” says Solomon.
What makes EMDR different
EMDR is based more on how a person reprocesses memories, rather than the strict plan of a therapist.
“The therapist facilitates movement with attuned bilateral stimulation and ‘stays out of the way’ as the distressing memory is shifting in an adaptive direction,” says Solomon. “Clients are able to find their own individualized and creative solutions and perspectives, in ways the clinician may never have thought of.”
A person undergoing EMDR doesn’t have to make themselves as vulnerable as they might during other forms of therapy. Sometimes not showing complete vulnerability makes things less taxing when undergoing treatment.
“The client does not have to describe the memory in detail. Not having to disclose shameful or humiliating moments may make it easier for some clients to engage in the therapeutic process,” Solomon explains.
The fact that EMDR is not a talk-based therapy is unique in that that, “EMDR goes to places where words don’t go and enables the processing of implicit, painful memories and their associated emotions and body sensations that talking alone does not seem to reach,” says Solomon.
EMDR success
When asked about a particular case in which EMDR helped a client overcome trauma, Solomon reflected on his experience with a police officer involved in the tragedy of the Sandy Hook Elementary School shooting:
“A police officer who was one of the first on-scene was very distressed by the images of children killed. For the next two years, he had nightmares and flashbacks, and found it difficult to be around children. He started the EMDR processing with an initial image of a dead child and an associated belief of ‘I’m helpless.’ With processing he realized he did the best he could at the situation. Next he remembered that many police officers from many different agencies started arriving. He realized that these policemen were off duty and coming on their own time to help out. When asked his thoughts/feelings about the incident, he said “UNITY,” and no longer felt distress. This session humbles me as to how the mind can find an adaptive way to deal with a horrible tragedy and I am grateful for EMDR therapy’s ability to help people.”
by Drake Baer, Senior writer at Thrive Global covering the brain and social sciences.
Teachers, parents and policymakers are finally started to realize that academic success depends on more than just “booksmarts,” the kind of fluid intelligence captured by IQ tests and the like. The importance of “soft” or “non-cognitive” skills like grit and emotional intelligence is growing rapidly. But there’s a deeper question here: where do these soft skills come from? According to a new paper in Psychological Science, it’s your mom.
The research team, lead by Lilian Dindo, a clinical psychologist at the Baylor College of Medicine, crossed disciplines and decades to discover what they describe as an “adaptive cascade” that happens in three parts, drawing a line from the relational experiences we have as infants to the academic achievements we have later on. “That having a supportive responsive caregiving environment can actually provide these inner resources that will foster something like effortful control, and that this in turn can actually promote better functioning in school is the new thing here,” she tells Thrive Global.
The first part of that cascade is “secure attachment.” Tots—in this study, one cohort of 9-month olds and another of two-to-three year olds—get strongly influenced by their primary caregivers, implicitly learning how relationships work (often called attachment in the psychology field).
In this study, the mothers rated their children’s security of attachment using a widely used assessment tool. “If a child is distressed and shows distress to a parent and the parent responds to the distress in sensitive and loving and reassuring ways the child then feels secure in their knowledge that they can freely express this negative emotion,” Dindo explained. “Learning in that way is very different than learning that if I express negative emotion then I will be rejected or minimized or ignored or ridiculed. And so the child will learn not to express the negative emotions, to inhibit that negative emotion, or to actually act up even more to try to get that response. Either way they’re learning that expressing this negative emotion will not be responded to in a sensitive or loving way.”
Think of it this way: if you ate at a restaurant and it made you sick, you’d be unlikely to go back; if you expressed hurt and your mom rejected it, you’d minimize that pain next time. Even very early in life, kids are already observing cause and effect.
Step two in the cascade is effortful control, or the ability to delay gratification and inhibit a response to something when it’s in your best interest to do so—it’s the toddler-aged forerunner of things like grit and conscientiousness. In this study, effortful control in toddlers was examined experimentally—for example, in a “snack delay” task where tykes are presented with a cup of Goldfish crackers and instructed to wait to eat them until the experimenter rings a bell—and through parental ratings of how well the kids controlled themselves at home.
Then comes the third part of the cascade: academic achievement. More than a decade after the first experiments, Dindo tracked down the mother-child duos. About two-thirds of each cohort participated in the follow-up, where moms sent in their now 11 to 15-year-old kids’ scores on a couple of academic different standardized tests. The researchers crunched the data from all of the experiments and found quite the developmental chain: secure attachment was associated with effortful control in toddlers, and in turn, effortful control at age 3 predicted better test scores in early adolescence.
While this study doesn’t explain the mechanics of that three-part cascade, Dindo thinks it has to do with how we learn to regard our own inner emotional lives from the way our moms (or primary caregivers) regard us. If mom is soothing and dependable, you learn to consistently do the same for yourself—you learn that you’re going to be okay even if you feel anxious in the moment, like when tackling homework or a test. To Dindo, this shows how coming from a psychologically or emotionally deprived environment can have long-term consequences: if you don’t get the loving attentiveness you need when you’re little, it’s going to be harder to succeed as you grow up.
In very hopeful news though, other studies out this year—like here (https://www.ncbi.nlm.nih.gov/pubmed/28401843) and here (https://www.ncbi.nlm.nih.gov/pubmed/28401847) —show that when parents get attachment interventions, or are coached to be more attentive to their toddlers, the kids’ effortful control scores go up, which should, in turn, lead to greater achievement down the line. Because as this line of research is starting to show, just like plants need sunlight to grow into their fullest forms, humans need skillful love to reach their full potential.
Psychol Sci. 2017 Oct 1:956797617721271. doi: 10.1177/0956797617721271. [Epub ahead of print]
Attachment and Effortful Control in Toddlerhood Predict Academic Achievement Over a Decade Later.
Dindo L, Brock RL, Aksan N, Gamez W, Kochanska G, Clark LA.
Abstract
A child’s attachment to his or her caregiver is central to the child’s development. However, current understanding of subtle, indirect, and complex long-term influences of attachment on various areas of functioning remains incomplete. Research has shown that (a) parent-child attachment influences the development of effortful control and that (b) effortful control influences academic success. The entire developmental cascade among these three constructs over many years, however, has rarely been examined. This article reports a multimethod, decade-long study that examined the influence of mother-child attachment and effortful control in toddlerhood on school achievement in early adolescence. Both attachment security and effortful control uniquely predicted academic achievement a decade later. Effortful control mediated the association between early attachment and school achievement during adolescence. This work suggests that attachment security triggers an adaptive cascade by promoting effortful control, a vital set of skills necessary for future academic success.
Recent findings suggest that treatment with psilocybin may “reset” brain connectivity in patients with treatment-resistant depression.
“Several of our patients described feeling ‘reset’ after the treatment and often used computer analogies. For example, one said he felt like his brain had been ‘defragged’ like a computer hard drive, and another said he felt ‘rebooted,’” Robin L. Carhart-Harris, PhD, of Imperial College London, said in a press release. “Psilocybin may be giving these individuals the temporary ‘kick start’ they need to break out of their depressive states and these imaging results do tentatively support a ‘reset’ analogy. Similar brain effects to these have been seen with electroconvulsive therapy.”
To assess psilocybin for treatment-resistant depression, researchers used functional MRI to measure cerebral blood flow (CBF) and blood oxygen-level dependent resting-state functional connectivity before and after psilocybin treatment among 16 patients with treatment-resistant depression.
One week after treatment, all patients exhibited decreased depressive symptoms.
At 5 weeks, 47% of the cohort met criteria for treatment response.
Whole-brain analyses indicated decreases in CBF in the temporal cortex, including the amygdala, following treatment with psilocybin.
Decreased CBF in the amygdala was associated with decreased depressive symptoms.
Posttreatment, resting-state functional connectivity was increased in the default-mode network.
Treatment response at 5 weeks was predicted by increased resting-state functional connectivity in the ventromedial prefrontal cortex-bilateral inferior lateral parietal cortex and decreased resting-state functional connectivity in the parahippocampal prefrontal cortex.
“Through collecting these imaging data we have been able to provide a window into the after effects of psilocybin treatment in the brains of patients with chronic depression,” Carhart-Harris said in the release. “Based on what we know from various brain imaging studies with psychedelics, as well as taking heed of what people say about their experiences, it may be that psychedelics do indeed ‘reset’ the brain networks associated with depression, effectively enabling them to be lifted from the depressed state.”
Carhart-Harris RL, et al. Sci Rep. 2017;doi:10.1038/s41598-017-13282-7.
Regular use of nicotine may normalize brain activity impairments linked with schizophrenia, according to a study using a mouse model, published online in Nature Medicine. The finding may explain why up to 90% of people with schizophrenia smoke—most of them heavily.
“Basically the nicotine is compensating for a genetically determined impairment,” said researcher Jerry Stitzel, PhD, of the University of Colorado Boulder. “No one has ever shown that before.”
Dr. Stitzel is part of an international research team that investigated whether a variant in the CHRNA5 gene, which is believed to increase schizophrenia risk, is associated with a reduction of neural firing in the brain’s prefrontal cortex, or hypofrontality. Researchers also examined whether nicotine could interrupt the effect.
In mice with the CHRNA5 gene variant, brain images confirmed hypofrontality, researchers reported. Behavioral tests further revealed that the mice shared key characteristics of people with schizophrenia, such as an inability to suppress a startle response and aversion to social interaction. The findings, they explained, suggest the CHRNA5 gene variant plays a role in schizophrenia by causing hypofrontality.
Nicotine, however, seemed to reverse hypofrontality. When researchers gave the mice daily nicotine, their sluggish brain activity improved within 2 days. Within a week, it was normal.
Researchers believe the nicotine corrected the impaired brain activity by acting on nicotinic receptors in regions important for healthy cognitive function.
Noting that hypofrontality is also linked with addiction, attention deficit hyperactivity disorder, bipolar disorder, and other psychiatric conditions, researchers believe the discovery could lead to new nonaddictive, nicotine-based medications.
“This defines a completely novel strategy for medication development,” said lead author Uwe Maskos, PhD, of Institut Pasteur, Paris, France.
—Jolynn Tumolo
References:
Koukouli F, Rooy M, Tziotis D, et al. Nicotine reverses hypofrontality in animal models of addiction and schizophrenia. Nature Medicine. 2017 January 23;[Epub ahead of print].
Nicotine normalizes brain deficits key to schizophrenia [press release]. Boulder, CO: University of Colorado Boulder; January 23, 2017.
Supplementation with taurine, the additive found in many energy drinks, may improve the symptoms in young people suffering a first episode of psychosis (FEP), according to a new study presented at the International Early Psychosis Association (IEPA) meeting.
Taurine, an amino acid naturally occurring in the body, exhibits an inhibitory neuro-modulatory effect in the nervous system and also functions as a neuroprotective agent. The authors devised a study to analyze the efficacy of taurine supplementation in improving symptoms and cognition in patients with FEP.
The study included 86 individuals with FEP between the ages of 18 and 25 years. It was conducted by Dr. Colin O’Donnell, Donegal Mental Health Service, Co. Donegal, Ireland, and Professor Patrick McGorry and Dr. Kelly Allott, Orygen, The National Centre of Excellence in Youth Mental Health, Australia, and colleagues. Each participant was taking a low dose antipsychotic medication and was attending Orygen.
Forty-seven participants received 4g of taurine daily, while 39 received placebo. Symptoms were assessed Using the scoring system called BPRS (Brief Psychiatric Rating Scale) and cognition was assessed with the MCCB tool (MATRICS consensus cognitive battery).
Results showed that taurine significantly improved symptoms on the BPRS scale, in overall score and in psychosis specific analysis, however, there was no difference between the treatment and placebo group regarding cognition. Depression symptoms (rated by the Calgary Depression Scale for Schizophrenia) and general overall functioning also improved in the taurine group.
“The use of taurine warrants further investigation in larger randomised studies, particularly early in the course of psychosis,” concluded the authors, who themselves, are planning to conduct further studies into the potential benefits of taurine in the treatment of psychosis.
St. Jude Children’s Research Hospital scientists have linked disruption of a brain circuit associated with schizophrenia to an age-related decline in levels of a single microRNA in one brain region
St. Jude Children’s Research Hospital scientists have identified a small RNA (microRNA) that may be essential to restoring normal function in a brain circuit associated with the “voices” and other hallucinations of schizophrenia. The microRNA provides a possible focus for antipsychotic drug development. The findings appear today in the journal Nature Medicine.
The work was done in a mouse model of a human disorder that is one of the genetic causes of schizophrenia. Building on previous St. Jude research, the results offer important new details about the molecular mechanism that disrupts the flow of information along a neural circuit connecting two brain regions involved in processing auditory information. The findings also provide clues about why psychotic symptoms of schizophrenia are often delayed until late adolescence or early adulthood.
“In 2014, we identified the specific circuit in the brain that is targeted by antipsychotic drugs. However, the existing antipsychotics also cause devastating side effects,” said corresponding author Stanislav Zakharenko, M.D., Ph.D., a member of the St. Jude Department of Developmental Neurobiology. “In this study, we identified the microRNA that is a key player in disruption of that circuit and showed that depletion of the microRNA was necessary and sufficient to inhibit normal functioning of the circuit in the mouse models.
“We also found evidence suggesting that the microRNA, named miR-338-3p, could be targeted for development of a new class of antipsychotic drugs with fewer side effects.”
There are more than 2,000 microRNAs whose function is to silence expression of particular genes and regulate the supply of the corresponding proteins. Working in a mouse model of 22q11 deletion syndrome, researchers identified miR-338-3p as the microRNA that regulates production of the protein D2 dopamine receptor (Drd2), which is the prime target of antipsychotics.
Individuals with the deletion syndrome are at risk for behavior problems as children. Between 23 and 43 percent develop schizophrenia, a severe chronic disorder that affects thinking, memory and behavior. Researchers at St. Jude are studying schizophrenia and other brain disorders to improve understanding of how normal brains develop, which provides insights into the origins of diseases like cancer.
The scientists reported that Drd2 increased in the brain’s auditory thalamus when levels of the microRNA declined. Previous research from Zakharenko’s laboratory linked elevated levels of Drd2 in the auditory thalamus to brain-circuit disruptions in the mutant mice. Investigators also reported that the protein was elevated in the same brain region of individuals with schizophrenia, but not healthy adults.
Individuals with the deletion syndrome are missing part of chromosome 22, which leaves them with one rather than the normal two copies of more than 25 genes. The missing genes included Dgcr8, which facilitates production of microRNAs.
Working in mice, researchers have now linked the 22q11 deletion syndrome and deletion of a single Dgcr8 gene to age-related declines in miR-338-3p in the auditory thalamus. The decline was associated with an increase in Drd2 and reduced signaling in the circuit that links the thalamus and auditory cortex, a brain region implicated in auditory hallucination. Levels of miR-338-3p were lower in the thalamus of individuals with schizophrenia compared to individuals of the same age and sex without the diagnosis.
The miR-338-3p depletion did not disrupt other brain circuits in the mutant mice, and the findings offer a possible explanation. Researchers found that miR-338-3p levels were higher in the thalamus than in other brain regions. In addition, miR-338-3p was one of the most abundant microRNAs present in the thalamus.
Replenishing levels of the microRNA in the auditory thalamus of mutant mice reduced Drd2 protein and restored the circuit to normal functioning. That suggests that the microRNA could be the basis for a new class of antipsychotic drugs that act in a more targeted manner with fewer side effects. Antipsychotic drugs, which target Drd2, also restored circuit function.
The findings provide insight into the age-related delay in the onset of schizophrenia symptoms. Researchers noted that microRNA levels declined with age in all mice, but that mutant mice began with lower levels of miR-338-3p. “A minimum level of the microRNA may be necessary to prevent excessive production of the Drd2 that disrupts the circuit,” Zakharenko said. “While miR-338-3p levels decline as normal mice age, levels may remain above the threshold necessary to prevent overexpression of the protein. In contrast, the deletion syndrome may leave mice at risk for dropping below that threshold.”
The study’s first authors are Sungkun Chun, Fei Du and Joby Westmoreland, all formerly of St. Jude. The other authors are Seung Baek Han, Yong-Dong Wang, Donnie Eddins, Ildar Bayazitov, Prakash Devaraju, Jing Yu, Marcia Mellado Lagarde and Kara Anderson, all of St. Jude.