Daily step counts between 5,000 to 10,000 or more reduced depression symptoms across 33 studies.
The associations may be due to several mechanisms, like improvement in sleep quality and inflammation.
Daily step counts of 5,000 or more corresponded with fewer depressive symptoms among adults, results of a systematic review and meta-analysis published in JAMA Network Open suggested.
The results are consistent with previous studies linking exercise to various risk reductions for mental health disorders and show that setting step goals “may be a promising and inclusive public health strategy for the prevention of depression,” the researchers wrote.
According to Bruno Bizzozero-Peroni, PhD, MPH, from Universidad De Castilla-La Mancha in Spain, and colleagues, daily step counts are a “simple and intuitive objective measure” of physical activity, while tracking such counts has become increasingly feasible for the general population thanks to the availability of fitness trackers.
“To our knowledge, the association between the number of daily steps measured
with wearable trackers and depression has not been previously examined through a meta-analytic approach,” they wrote.
The researchers searched multiple databases for analyses assessing the effects of daily step counts on depressive symptoms, ultimately including a total of 27 cross-sectional studies and six longitudinal studies comprising 96,173 adults aged 18 years or older.
They found that in the cross-sectional studies, daily step counts of 10,000 or more (standardized mean difference [SMD] = 0.26; 95% CI, 0.38 to 0.14), 7,500 to 9,999 (SMD = 0.27; 95% CI, 0.43 to 0.11) and 5,000 to 7,499 (SMD = 0.17; 95% CI, 0.3 to 0.04) corresponded with reduced depressive symptoms vs. daily step counts less than 5,000.
In the prospective cohort studies, people with 7,000 or more steps a day had a reduced risk for depression vs. with people with fewer than 7,000 daily steps (RR = 0.69; 95% CI, 0.62-0.77), whereas an increase of 1,000 steps a day suggested an association with a lower risk for depression (RR = 0.91; 95% CI, 0.87-0.94).
There were a couple study limitations. The researchers noted that reverse associations are possible, while they could not rule out residual confounders.
They also pointed out that there are some remaining questions, such as whether there is a ceiling limit after which further step counts would no longer reduce the risk for depression.
Bizzozero-Peroni and colleagues highlighted several possible biological and psychosocial mechanisms behind the associations, like changes in sleep quality, inflammation, social support, self-esteem, neuroplasticity and self-efficacy.
They concluded that “a daily active lifestyle may be a crucial factor in regulating and reinforcing these pathways” regardless of the exact combination of mechanisms responsible for the positive link.
“Specifically designed experimental studies are still needed to explore whether there are optimal and maximal step counts for specific population subgroups,” they wrote.
The genetic mutation that causes Huntington’s disease (HD)—a devastating brain disease that disrupts mobility and diminishes cognitive ability—may also enhance early brain development and play a role in promoting human intelligence.
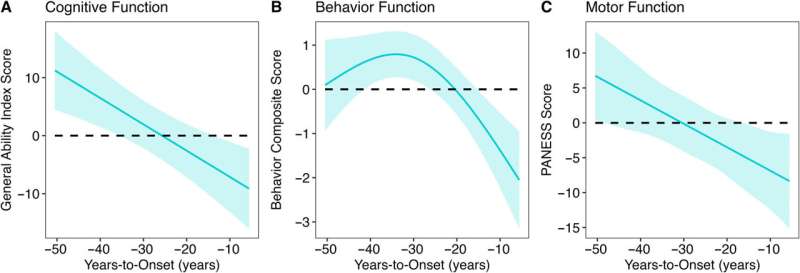
This revelation comes from more than 10 years of brain imaging and brain function data, including motor, cognitive, and behavioral assessments, collected from a unique population—children and young adults who carry the gene for HD. While an HD mutation will eventually cause fatal brain disease in adulthood, the study finds that early in life, children with the HD mutation have bigger brains and higher IQ than children without the mutation.
“The finding suggests that early in life, the gene mutation is actually beneficial to brain development, but that early benefit later becomes a liability,” says Peg Nopoulos, MD, professor and head of psychiatry at the UI Carver College of Medicine, and senior author on the study published in The Annals of Neurology.
The finding may also have implications for developing effective treatments for HD. If the gene’s early action is beneficial, then simply aiming to knock out the gene might result in loss of the developmental benefit, too. Creating therapies that can disrupt the gene’s activity later in the patient’s lifetime might be more useful.
The new data about the gene’s positive effect on early brain development is also exciting to Nopoulos for another reason.
“We are very interested in the fact that this appears to be a gene that drives IQ,” she says. “No previous study has found any gene of significant effect on IQ, even though we know intelligence is heritable.”
HD gene linked to better brain development in early life
Huntington’s disease is caused by a mutation in the huntingtin (HTT) gene. The protein produced by the HTT gene is necessary for normal development, but variations within a segment of the protein have a profound effect on the brain.
The segment in question is a long repeat of one amino acid called glutamine. More repeats are associated with bigger, more complex brains. For example, species such as sea urchins or fish have no repeats, but these repeats start to appear higher up the evolutionary ladder. Rodents have a few repeats, while apes (our closest relatives) have even more repeats; and humans have the most.
Most people have repeats in the range of 10–26, but if a person has 40 or more repeats, then they develop HD. Although the gene expansion is present before birth, HD symptoms do not appear until middle age. Nopoulos’s team at the University of Iowa has a long history of studying how the HTT gene expansion affects brain development in the decades before disease onset.
“We know that the expanded gene causes a horrible degenerative disease later in life, but we also know it is a gene that is crucial for general development,” she says.
“We were surprised to find that it does have a positive effect on brain development early in life. Those who have the gene expansion have an enhanced brain with larger volumes of the cerebrum and higher IQ compared to those who don’t.”
In particular, the study found that decades before HD symptoms appeared, children with the HD gene expansion showed significantly better cognitive, behavioral, and motor scores compared to children with repeats within the normal range. Children with the expanded gene also had larger cerebral volumes and greater cortical surface area and folding. After this initial peak, a prolonged deterioration was seen in both brain function and structure.
The study gathered this data by following almost 200 participants in the Kids-HD study, the only longitudinal study of children and young adults at risk for HD due to having a parent or grandparent with the disease.
Evolutionary benefit comes at a cost
Although surprising, the findings are in line with studies by evolutionary biologists who believe that genes like HTT may have been “positively selected” for human brain evolution. This theory, known as antagonistic pleiotropy, suggests that certain genes can produce a beneficial effect early in life, but come at a cost later in life.
The finding also challenges the idea that the protein produced by the HD gene is solely a toxic protein that causes brain degeneration.
“Overall, our study suggests that we should rethink the notion of the toxic protein theory,” says Nopoulos, who is also a member of the Iowa Neuroscience Institute.
“Instead, we should consider the theory of antagonistic pleiotropy—a theory that suggests that genes like HTT build a better brain early in life, but the cost of the superior brain is that it isn’t built to last and may be prone to premature or accelerating aging.
“This means that instead of knocking down the gene for therapy, drugs that slow the aging process may be more effective.”
Next steps
Nopoulos’s team is already making progress extending the research from the Kids-HD program. Nopoulos has established the Children to Adult Neurodevelopment in Gene-Expanded Huntington’s Disease (ChANGE-HD), a multi-site study that aims to recruit hundreds of participants for a total of over 1,200 assessments to validate the key findings from the Kids-HD study and to enhance future research on HD.
A primary area of focus will be understanding how an enlarged brain can later lead to degeneration. One hypothesis Nopoulos and her team will explore involves the idea that an enlarged cortex might produce excess glutamate (an important neurotransmitter), which is beneficial in early brain development, but later leads to neurotoxicity and brain degeneration.
In addition to Nopoulos, the UI team included Mohit Neema, MD, UI research scientist and first author of the study; Jordan Schultz, PharmD; Douglas Langbehn, MD, Ph.D.; Amy Conrad, Ph.D.; Eric Epping, MD, Ph.D.; and Vincent Magnotta, Ph.D.
More information: Mohit Neema et al, Mutant Huntingtin Drives Development of an Advantageous Brain Early in Life: Evidence in Support of Antagonistic Pleiotropy, Annals of Neurology (2024). DOI: 10.1002/ana.27046
University at Buffalo neuroscientists have identified the binding site of low-dose ketamine, providing critical insight into how the medication, often described as a wonder drug, alleviates symptoms of major depression in as little as a few hours with effects lasting for several days.
Published in Molecular Psychiatry, the UB discovery will also help scientists identify how depression originates in the brain, and will stimulate research into using ketamine and ketamine-like drugs for other brain disorders.
A lifesaving drug
Ketamine has been used since the 1960s as an anesthetic, but in 2000, the first trial of far lower doses of ketamine proved its rapid efficacy in treating major depression and suicidal ideation.
“Due to its fast and long-lasting effects, low-dose ketamine proved to be literally a lifesaving medicine,” says Gabriela K. Popescu, Ph.D., senior author on the research and professor of biochemistry in the Jacobs School of Medicine and Biomedical Sciences at UB.
Traditional antidepressants take months to kick in, which increases the risk for some patients to act on suicidal thoughts during the initial period of treatment. Ketamine provides almost instant relief from depressive symptoms and remains effective for several days and up to a week after administration. Since this observation was published in the early 2000s, ketamine clinics, where the drug is administered intravenously to treat depression, have been established in cities nationwide.
But just how ketamine achieves such a dramatic antidepressive effect so quickly has been poorly understood at the molecular level. This information is critical to understanding not only how best to use ketamine, but also to developing similar drugs.
Selective effects on NMDA receptors
Ketamine binds to a class of neurotransmitter receptors called N-methyl-D-aspartate (NMDA) receptors. Popescu is an expert on how these receptors produce electrical signals that are essential for cognition, learning and memory, and how these signals, when dysregulated, result in psychiatric symptoms.
“We demonstrate in this article how ketamine at very low concentrations can affect the activity of only select populations of NMDA receptors,” says Popescu
NMDA receptors are present throughout the brain and are essential for maintaining consciousness. For this reason, she explains, drugs that act indiscriminately on all NMDA receptors have unacceptable psychiatric side effects.
“We believe that the selectivity we uncovered in our research explains how low-dose ketamine can treat major depression and prevent suicides in people with depression,” Popescu says.
The research was sparked by an observation in her lab by co-author Sheila Gupta, then a UB undergraduate. “Sheila noticed that when applied onto NMDA receptors that were chronically active, ketamine had a stronger inhibitory effect than expected based on the literature,” Popescu explains. “We were curious about this discrepancy.”
Back when ketamine’s antidepressant effects first became known, researchers tried to find out how it worked by applying it onto synaptic currents produced by NMDA receptors, but the drug produced little or no effect.
“This observation caused many experts to turn their attention to receptors located outside synapses, which might be mediating ketamine’s antidepressive effects,” Popescu says.
“Sheila’s observation that ketamine is a stronger inhibitor of receptors that are active for longer durations inspired us to look for mechanisms other than the direct current block, which was assumed to be the only effect of ketamine on NMDA receptors.”
Few labs with this NMDA expertise
Popescu’s lab is among a handful in the world with the expertise to quantify the process by which NMDA receptors become active. This allowed Popescu and her colleagues to identify and measure what exactly changed during the NMDA activations when ketamine was present at very low doses versus when it was present at high (anesthetic) doses.
“Because we track activity from a single receptor molecule over an extended period of time, we can chart the entire behavioral repertoire of each receptor and can identify which part of the process is altered when the receptor binds a drug or when it harbors a mutation,” Popescu explains.
“The mechanism we uncovered suggests that at low doses, ketamine will only affect the current carried by receptors that had been active in the background for a while, but not by synaptic receptors, which experience only brief, intermittent activations,” she continues.
“This results in an immediate increase in excitatory transmission, which in turn lifts depressive symptoms. Moreover, the increase in excitation initiates the formation of new or stronger synapses, which serve to maintain higher excitatory levels even after ketamine has cleared from the body, thus accounting for the long-term relief observed in patients.”
The UB research helps explain why such low doses of ketamine are effective.
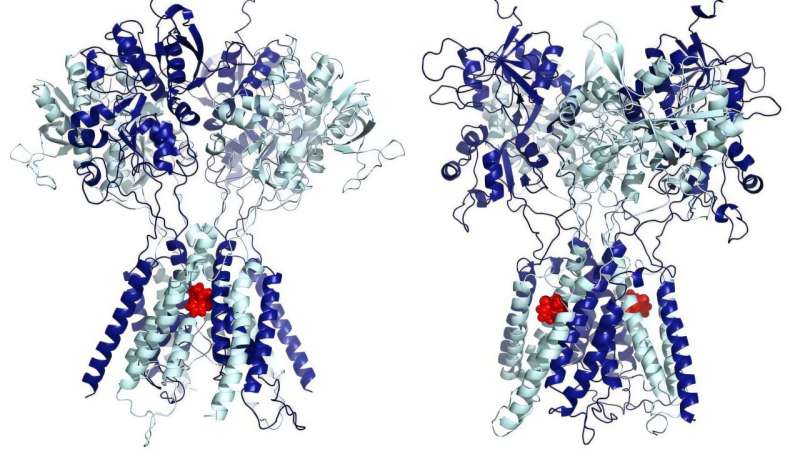
“Our results show that very low levels of ketamine, on the nanoscale, are sufficient to fill two lateral grooves of the NMDA receptors to selectively slow down extra-synaptic receptors, alleviating depression. Increasing the dose causes ketamine to spill over from the grooves into the pore and begin to block synaptic currents, initiating the anesthetic effect,” says Popescu.
Popescu’s co-authors in the Department of Physics in the College of Arts and Sciences simulated the three-dimensional structure of the NMDA receptor and predicted the exact residues to which ketamine binds in the lateral sites.
“These interactions are strong and account for the high affinity of the receptor for low doses of ketamine,” she says.
“The simulations show that at high concentrations, which is how it is used as an anesthetic, ketamine indeed lodges itself in the central ion-conducting pore of the receptors, where it stops ionic current from flowing through the receptor,” says Popescu.
In contrast, at low concentrations, ketamine functions very differently, attaching to two symmetrical sites on the sides of the pore, such that instead of stopping the current, ketamine makes receptors slower to open, reducing the current only a little bit.
“Finding the exact binding site on the receptor offers the perfect template for developing ketamine-like drugs that could be administered orally and may lack the addictive potential of ketamine,” says Popescu.
The natural next step is to screen existing drugs that can fit in the lateral grooves of NMDA receptors, first computationally and then experimentally.
More information: Jamie A. Abbott et al, Allosteric inhibition of NMDA receptors by low dose ketamine, Molecular Psychiatry (2024). DOI: 10.1038/s41380-024-02729-9
A non-deceptive placebo injection reduced chronic back pain with effect size similar to typical treatments.
Secondary outcome benefits and brain changes lasted up to 1 year.
A single saline injection, openly prescribed as a placebo, yielded approximately 1 month of chronic back pain improvement, along with longer-term benefits in depression and sleep, according to data published in JAMA Network Open.
“We have known that placebos can be powerful pain relievers, but it has been unclear how to use them ethically, without patient deception,” Yoni K. Ashar, PhD, assistant professor at the University of Colorado Anschutz Medical Campus, told Healio. “This spurred the development of the ‘open label,’ non-deceptive placebo treatment, which we studied here.”
To investigate the long-term efficacy of open label placebo in chronic back pain, Ashar and colleagues recruited 101 adults (mean age, 40.4 years) with moderate chronic back pain from the Boulder, Colorado, area between November 2017 and August 2018, with a follow-up at 1 year.
Trial participants were randomly assigned to either continue their usual care alone or to also receive a single, open label lumbar saline injection, along with information about how the placebo effect can lead to pain relief. The primary outcome was average pain over the last week 1 month after treatment, measured using a scale of 0 to 10. Secondary outcomes also assessed pain interference, depression, anxiety, anger and sleep quality.
At 1 month, those who received placebo injections reported greater reductions in chronic back pain than the usual care group (relative reduction, 0.61; Hedges g = 0.45; 95% CI, –0.89 to 0.04), according to the researchers.
By 1 year post-treatment, the between-group difference in pain relief was reduced to insignificance. However, after 1 month, other significant benefits were seen in depression, anger, anxiety and sleep disruption, with “medium sized” effect sizes ranging from 0.3 to 0.5 (P < .03 for all).
The researchers also compared neuroimaging between the groups. Functional MRI scans were taken as participants performed both an “evoked” back pain procedure, which used an inflating balloon to cause back distention and pain, and a “spontaneous” pain procedure, where patients rated their pain once per minute over the course of an 8-minute scan.
Overall, the neuroimaging showed “altered brain responses to evoked back pain and altered functional connectivity during spontaneous pain consistent with engagement of descending modulatory pain pathways,” Ashar and colleagues wrote.
The researchers described the placebo injection’s pain relief benefit as “modest in magnitude” but clinically significant and comparable with the effect sizes of typical treatments such as NSAIDs, but with fewer adverse events.
“These findings speak to the power of healing rituals, even when we know they are healing rituals,” Ashar said. “Although we view this study as more mechanistic and conceptually provocative than as clinically applicable, it suggests that providers may be able to ethically prescribe a placebo for their patients one day, without deception. In addition, the duration of benefits on secondary outcomes and the observed brain changes were surprising, considering how brief and minimalist the intervention was.”
Fear strikes in many forms – standing on the edge of a towering skyscraper, glimpsing a tarantula, or feeling your heart race as you prepare to deliver a speech.
The scientific community long believed these scenarios stimulated brains similarly.
“There’s this story that we’ve had in the literature that the brain regions that predict fear are things like the amygdala, or the orbital frontal cortex area, or the brainstem,” said Ajay Satpute, an associate professor of psychology at Northeastern University.
“Those are thought to be part of a so-called ‘fear circuit’ that’s been a very dominant model in neuroscience for decades.”
Challenging the fear circuit model
In early October 2024, Satpute and his team released a study challenging this long-held belief.
The researchers used MRI scans to examine the brain’s response to three distinct fear-inducing scenarios: fear of heights, spiders, and public speaking.
Contrary to prior assumptions, the study revealed each type of fear activated different brain regions, debunking the idea of a universal “fear circuit.”
“Much of the debate on the nature of emotion concerns the uniformity or heterogeneity of representation for particular emotion categories,” noted the researchers.
The team discovered that “the overwhelming majority of brain regions that predict fear only do so for certain situations.”
Research suggests responses to fear are more specific than previously thought. These findings carry important implications for understanding anxiety across species, and how to develop neural signatures for personalized treatments.
Machine learning and fear in the brain
The research tested long-standing assumptions about how fear works, particularly as neuroscience increasingly relies on AI and machine learning to predict emotions.
“Most of those approaches assume that there is a single pattern that underlies the brain-behavior relationship: there’s a single pattern that predicts disgust. There’s a single pattern that predicts anger,” said Satpute.
“Well, if that’s true, then such a pattern should be apparent for different varieties of fear.”
However, when it comes to fear, the study showed a more complex picture.
Focus of the research
In the experiment, the researchers asked 21 participants to identify their fears and used magnetic resonance imaging (MRI) scans to monitor brain activity as they watched videos depicting anxiety-inducing scenarios.
“We tried to find really scary videos of spiders,” Satpute said. “Because I don’t want a neural predictive model that ‘says you’re looking at a spider.’ I want a neural predictive model that says ‘you’re experiencing fear.’”
Revealing fear’s hidden complexities
Following each video, participants rated their levels of fear, valence (how pleasant or unpleasant the experience was), and arousal on a questionnaire.
The study revealed two surprising insights: responses were observed in a wider array of brain regions and not all brain regions were involved across all scenarios.
“The amygdala, for instance, seemed to carry information that predicted fear during the heights context, but not some of the other contexts,” Satpute said. “We’re not seeing these so-called ‘classic threat areas’ involved in being predictive of fear across situations.”
Body’s response to emotional triggers
The research is part of a broader body of work from Satpute’s lab, which focuses on understanding how fear manifests in the body.
In a previous 2021 study, the team explored physiological responses to fear such as sweat and heart rate when facing different triggers like heights or confrontations with law enforcement.
The study also revealed that different triggers caused varied bodily reactions, supporting the idea that fear isn’t one-size-fits-all.
Implications for future treatments
Satpute hopes to replicate these findings with a larger and more diverse participant pool and factoring in demographics like age and gender.
While the current study has a small sample size, the results could reshape how health professionals approach treating fear and anxiety disorders.
“When we look at the brain and the neural correlates of fear, part of the reason we want to understand is so we can intervene on it,” noted Satpute. “Our findings suggest the interventions might also need to be tailored to the person and situation.”
Revolutionizing fear-based therapies
This shift in understanding could revolutionize behavior-based therapies for conditions like phobias and PTSD. It might even impact drug-based treatments.
“Drug-based therapies that target a particular circuit do work, but only for about fiftyish percent of people,” Satpute said. “It’s not really clear why.”
“Our research offers at least some explanation – the brain regions that are going to matter for any emotional experience are going to vary by the person and situation. If you focus only on what’s common, you ignore so much.”
This understanding of fear moves beyond the idea of a “fear circuit” and opens doors for personalized treatments.
Whether it’s the fear of falling, facing a spider, or standing in front of an audience, the research shows fear is more complex than once believed.
Summary: New research shows that the brain divides the day into “chapters” based on what a person focuses on. These mental boundaries aren’t solely prompted by changes in surroundings but also by internal goals and priorities. In experiments using audio narratives, participants’ brains organized events differently depending on whether they focused on specific details.
This study suggests that how we experience and remember events is influenced by both context and what matters most to us at the time.
Key Facts:
The brain forms new “chapters” based on attention and personal goals, not just environment.
MRI scans showed that people segmented stories differently depending on their focus.
The research may help explain how expectations influence memory formation.
Source: Columbia University
The moment a person steps off the street and into a restaurant—to take just one example—the brain mentally starts a new “chapter” of the day, a change that causes a big shift in brain activity. Shifts like this happen all day long, as people encounter new environments, like going out for lunch, attending their kid’s soccer game, or settling in for a night of watching TV.
But what determines how the brain divides the day into individual events that we can understand and remember separately?
That’s what a new paper in the journal Current Biology aimed to find out.
The research team, led by Christopher Baldassano, an associate professor of Psychology, and Alexandra De Soares, then a member of his lab, turned up interesting results.
The researchers wanted to better understand what prompts the brain to form a boundary around the events we encounter, effectively registering it as a new “chapter” in the day.
One possibility is that new chapters are entirely caused by big changes in a person’s surroundings, like how walking into a restaurant takes them from outdoors to indoors.
Another possibility, however, is that the new chapters are prompted by internal scripts that our brain writes based on past experience, and that even big environmental changes might be ignored by our brain if they are not related to our current priorities and goals.
To test their hypothesis, researchers developed a set of 16 audio narratives, each about three to four minutes long. Each narrative took place in one of four locations (a restaurant, an airport, a grocery store, and a lecture hall) and dealt with one of four social situations (a breakup, a proposal, a business deal, and a meet cute).
The researchers found that the way the brain divides up an experience into individual events depends on what a person currently cares about and is paying attention to.
When listening to a story about a marriage proposal at a restaurant, for example, subjects’ prefrontal cortex would usually be organizing the story into events related to the proposal, leading up (hopefully) to the final “yes.”
But the researchers found that they could force the prefrontal cortex to organize the story in a different way if they instead asked study participants to focus on the events related to the dinner orders of the couple. For study participants who were told to focus on these details, moments like ordering dishes became critical new chapters in the story.
“We wanted to challenge the theory that the sudden shifts in brain activity when we start a new chapter of our day are only being caused by sudden shifts in the world—that the brain isn’t really ‘doing’ anything interesting when it creates new chapters, it’s just responding passively to a change in sensory inputs,” Baldassano said.
“Our research found that isn’t the case: The brain is, in fact, actively organizing our life experiences into chunks that are meaningful to us.”
The researchers measured where the brain created new chapters both by looking at MRI scans of the brain to identify fresh brain activity, and, in a separate group of participants, by asking them to press a button to indicate when they thought a new part of the story had begun.
They found that the brain divided stories into separate chapters depending on the perspective they were told to be attuned to—and it didn’t just apply to the proposal-in-a-restaurant scenario: A person hearing a story about a breakup in an airport could, if prompted to pay attention to details of the airport experience, register new chapters as they went through security and arrived at their gate.
Meanwhile, a person who heard a story about a person closing a business deal while grocery shopping could be prompted to register either the new steps of the business deal as new chapters, or to be attuned primarily to the phases of grocery shopping instead.
The details that the study participants were prompted to pay attention to influenced what their brain perceived as a new chapter in the story.
Moving forward, the researchers hope to investigate the impact that expectations have on long-term memory. As part of this study, the researchers also asked each participant to tell them everything they remembered about each story.
They are still in the process of analyzing the data to understand how the perspective they were asked to adopt while listening to the story changes the way they remember it. More broadly, this study is part of an ongoing effort in the field to build a comprehensive theory about how real-life experiences are divided up into event memories.
The results indicate that prior knowledge and expectations are a key ingredient in how this cognitive system works.
Baldassano described the work as a passion project.
“Tracking activity patterns in the brain over time is a big challenge that requires using complex analysis tools,” he said: “Using meaningful stories and mathematical models to discover something new about cognition is exactly the kind of unconventional research in my lab that I am most proud of and excited about.”
Serotonin is often referred to as the “happiness molecule.” It plays a critical role in affecting mood levels and is also a neurotransmitter that sends signals within the brain and the body.
Researchers have generally thought that the chemical plays a global role in modulating brain states by acting over a longer timescale than dopamine, which signals reward but operates on a much shorter timeframe.
Now, a Dartmouth study published in The Journal of Neuroscience reports that serotonin increases in anticipation of a reward and scales with the value of that reward.
For decades, prior research has looked at the release of dopamine levels in encoding the value of rewards at a subsecond timescale using a technique that enabled scientists to monitor it throughout different areas in the mouse brain.
Techniques for monitoring serotonin at this timescale did not previously exist, leaving many unknowns about when serotonin is released in the brain because of its widespread projections. Serotonin is an extraordinarily complex system, with the cells located in one small region of the brain, which then send their messages to pretty much every other area of the brain.
There are 14 serotonin receptors, which are like 14 different locks and the key, serotonin, can fit into any one of those locks, unlocking a different message depending on the door. This explains why past studies have focused on targeting those receptors before it was possible to examine serotonin itself.
“In this research we used a new biosensor called GRAB-serotonin, for short, that could, for the first time, measure the molecule by ‘grabbing’ serotonin released in the brain, while the mouse was running around receiving a tasty treat,” says senior author Kate Nautiyal, an assistant professor of psychological and brain sciences at Dartmouth.
Using a technique called fiber photometry, light can be used to trigger and then measure fluorescence fluctuations from a biosensor like GRAB, whenever serotonin is detected. The team was able to study the release of serotonin in mice while they received rewards, which in this case were varied concentrations of evaporated milk, which mice love. The researchers were then able to look at how serotonin levels changed depending on how good the reward was.
“We had a pretty good understanding that if you alter serotonin signaling by targeting receptors or manipulating reuptake such as with selective serotonin reuptake inhibitors, which are used in antidepressants, you get these broad impacts on mood and can change the way that animals or individuals seem to regulate behavior,” says co-author Mitchell Spring, a postdoctoral researcher who worked on this project in the Nautiyal Lab, a behavioral neuroscience lab in the Department of Psychological and Brain Sciences at Dartmouth.
The results showed that consumption of higher concentrations of the reward was associated with greater serotonin release. When the mice were thirsty and were given water, there was a big serotonin signal, and when they were satiated with a good reward and were full, the serotonin signal was not as strong.
The findings also showed that if you give mice a cue that predicts the reward, serotonin levels rise during the cue, or anticipation, of the reward.
“We found that you can modulate the serotonin signal with the subjective value of the reward,” says Nautiyal. “Our results tell us that serotonin is really a signal in the brain monitoring how good a reward is.”
In measuring the release of serotonin, the team focused on one brain region, the dorsomedial striatum, which has previously been associated very strongly with dopamine, decision-making, and impulsivity.
The researchers say that selective serotonin reuptake inhibitors are widely prescribed and generally effective but we don’t fully understand how they work or what serotonin is doing to address the behaviors that these antidepressants are treating.
“A better understanding of how serotonin is operating at baseline or in healthy individuals during a positive experience could be used to develop more targeted treatments for psychiatric disorders like depression and addiction,” says Nautiyal.
More information: Mitchell G. Spring et al, Striatal serotonin release signals reward value, The Journal of Neuroscience (2024). DOI: 10.1523/JNEUROSCI.0602-24.2024
Prescribing rates for stimulants that treat attention-deficit/hyperactivity disorder (ADHD) have increased significantly over the past decade, with some of the largest increases reported during the COVID-19 pandemic. A new study of adult emergency department admissions at Mass General Brigham, led by McLean Hospital researchers, found that individuals who are taking high doses of amphetamine (e.g. Adderall) face more than a five-fold increased risk for developing psychosis or mania. Findings were published September 12th in the American Journal of Psychiatry.
Overall, individuals with past-month prescription amphetamine use had a greater likelihood of new-onset psychosis or mania than individuals without past-month use. The risk was highest in those taking 30 mg or more of dextroamphetamine (which corresponds to 40 mg of Adderall), according to the study.
Previous studies have linked stimulants to psychosis and mania risk; however, information had been lacking on whether dosing impacted risk.
“Stimulant medications don’t have an upper dose limit on their labels, and our results show that it is clear that dose is a factor in psychosis risk and should be a chief consideration when prescribing stimulants,” said lead study author Lauren Moran, MD, a pharmacoepidemiology researcher at McLean Hospital. “This is a rare but serious side effect that should be monitored by both patients and their doctors whenever these medications are prescribed.”
Moran said the study was born out of her past clinical observations as an inpatient psychiatrist. She and her McLean colleagues would regularly see patients coming in experiencing first episodes of psychosis, and their medical records would reveal they were prescribed high doses of stimulants by their doctors.
Researchers reviewed electronic health records of Mass General Brigham patient encounters between 2005 and 2019, focusing on adults aged 16 to 35, the typical age of onset for psychosis and schizophrenia. All patients were admitted to McLean Hospital following referrals from other hospitals in the Mass General Brigham healthcare system. The researchers identified 1,374 cases of individuals presenting with first-episode psychosis or mania, compared to 2,748 control patients with a psychiatric hospitalization for other conditions like depression or anxiety. They conducted a comparison analysis of stimulant use over the preceding month and accounted for other factors, including substance use, in order to isolate the effects of stimulants.
They found the attributable risk percentage among those exposed to any prescription amphetamine was nearly 63% and for high dose amphetamine was 81%. These findings suggest that among people who take prescription amphetamine, 81% of cases of psychosis or mania could have been eliminated if they were not on the high dose. While a significant dose-related risk increase was seen in patients taking high doses of amphetamine, no significant risk increase was seen with methylphenidate (Ritalin) use, which is consistent with previous research, including a 2019 study led by Moran.
While the study does not prove causality, the researchers note there is a plausible biological mechanism in neurobiological changes that include a release of higher levels of the neurotransmitter dopamine from amphetamines, that parallel dopaminergic changes observed in psychosis.
Limitations of the study include inconsistencies with how electronic health records are kept. Additionally, with the research taking place in a psychiatric hospital in the Boston area that sees many patients with psychosis, it may make these findings less generalizable to other parts of the country.
Moran said the findings need not create alarm but should lead to extra caution when these medications are prescribed, especially for those who have risk factors for psychosis and mania.
“There’s limited evidence that prescription amphetamines are more effective in high doses,” said Moran. “Physicians should consider other medications our study found to be less risky, especially if a patient is at high risk for psychosis or mania.”
Authorship: In addition to Moran, Mass General Brigham co-authors included Joseph P. Skinner, BA (BWH), Ann K. Shinn MD, MPH (McLean), Kathryn Nielsen (McLean), Vinod Rao, MD, PhD (MGH), Trevor Taylor, MD, MPH (MGH), Talia R. Cohen (McLean), Cemre Erkol, MD (McLean), Jaisal Merchant, MA (McLean), Christin A. Mujica, MA (McLean), Roy H. Perlis, MD, MSc, (MGH) and Dost Ongur, MD, PhD (McLean).
Funding: This work was funded by a grant from the National Institute of Mental Health (NIMH), R01 MH122427.
Disclosures: Perlis received personal fees from Genomind, Burrage Capital, Psy Therapeutics Inc, Circular Genomics Inc, and Vault Health unrelated to the submitted work. Dr. Ongur received honorariums for scientific presentations to Neumora Inc. and Guggenheim LLC unrelated to the submitted work. Dr. Moran is employed by Sage Therapeutics (unrelated to this work and after study completed and submitted for publication). All other authors report no financial relationships with commercial interests.
Paper cited: Moran, LV et al. “Risk of Incident Psychosis and Mania with Prescription Amphetamines,” American Journal of Psychiatry. DOI: 10.1176/appi.ajp.20230329
New data revealed that health insurance coverage, internet access and income level can influence suicide risk.
PCPs should create a comfortable environment to address these factors and reduce suicide risk.
By addressing factors like health insurance coverage, internet access and income level, primary care providers can play an important role in suicide prevention, according to experts.
“September is Suicide Prevention Month and today is World Suicide Prevention Day, a day where we raise awareness and attention to this issue, emphasizing the message that suicide is preventable,” Debra Houry, MD, MPH, CDC’s Chief Medical Officer, said in a media briefing on Sept. 10. “Suicide rates have increased over the last 20 years and remain high: more than 49,000 people died by suicide in 2022, and provisional data indicate a similar number of people died by suicide in 2023.”
By addressing factors like health insurance coverage, internet access and income level, PCPs can play an important role in suicide prevention, according to experts. Image: CDC
Brent Smith, MD, MSc, MLS, FAAFP, a family physician in Mississippi and member of the American Academy of Family Physicians board of directors, told Healio that PCPs “play a really underappreciated, undervalued role in all mental health care, but specifically suicide prevention.”
“Family physicians often become the de facto treatment for mental health because they’re the ones that are already established with the patient, that are available, and that have established a patient’s trust, and therefore kind of have a unique window,” he said.
Although suicide prevention often focuses on helping patients in crisis, Houry said it is also vital to reduce factors that lead to increased suicide risk and actively address factors that promote resilience, “to keep people from ever getting to a crisis.”
In that vein, a new CDC vital signs report highlighted the importance of exploring community factors — particularly, health insurance coverage, household income levels and broadband internet access — that could be improved to help prevent suicides.
“We all likely know someone who has struggled with suicidal thoughts,” Houry said. “I lost two medical school classmates to suicide and know how this crisis can truly impact anyone and everyone.”
The new data
Alison Cammack, PhD, MPH, lead author of the new vital signs report, and colleagues found that suicide rates were lowest for counties with higher levels of household income, broadband internet access and health insurance coverage.
More specifically, when compared with the counties that had the lowest levels of these factors, suicide rates were:
13% lower in counties with the most household income;
26% lower in counties with the highest health insurance coverage; and
44% lower in counties where most of the homes have broadband internet access.
Cammack said there could be many reasons as to why this may be the case.
“We know that these three factors are linked with protective factors that have been shown to help reduce the risk of suicide,” Cammack, who is also health scientist of the CDC Suicide Prevention Team, said. “Health insurance coverage can help [patients] access mental health and primary care services and treatment; high-speed Internet access connects people to prevention resources, job opportunities, telehealth services and friends and family; and household financial resources such as income and economic support put in place by local state and federal governments can help families secure food, housing, health care and other basic needs.”
The report also found some groups continue to face higher suicide rates, Cammack added, including men, people in rural areas, white people and American Indian/Alaskan Native people.
“It is important to note that many barriers challenge a person’s ability to access health insurance, broadband internet and higher income,” she said. “For example, tribal and rural communities may lack the infrastructure to obtain internet access. It’s imperative that our nation works toward a comprehensive suicide prevention approach focused on programs, practices and policies designed to prevent suicide crises before they happen.”
For patients who are already stressed by these community-level factors, “it does not take much other stress to really put you in a bad place from a mental health standpoint,” Smith said.
“All of the things that we can’t control with medicine … Those social determinants play as much of a role as anything else,” he said. “And you can throw medicine [at symptoms] all you want, but we still have to treat the other things that the patients deal with.”
Importance for PCPs
Better understanding factors that influence suicide risk can improve prevention efforts and ultimately save more lives, Houry said.
“Suicide is preventable, and we know what works to stop it and to spare families and friends from losing loved ones,” she said.
PCPs must prioritize evaluating and treating these and other social factors that can impact patient health, Smith said.
“Move social determinants of health higher up in your priority list when you’re dealing with mental health, suicide and other issues,” he said. “Come to it sooner, address it quicker, and make it as much of a priority as you can in your treatment plans, in order to have a more lasting impact and more success in treating these types of things.”
That can start with creating a positive environment where patients feel safe in talking about mental health, he said.
“The biggest thing for you to do is just make the environment comfortable for people to talk about the things that are really bothering them, and then you’ll start to see some actual impact on this,” Smith said. “The problem is just making sure we’re putting it into perspective. We often undervalue how much these social stressors drive their other issues.”
Smith acknowledged that PCPs are often unable to address social determinants of health until they have tried therapy, medicine and other treatment modalities. If they do prioritize addressing these factors, “they’ll find that they’re more successful getting not only their mental health issues under control, but also their chronic medical problems,” he added.
“Our work to make patients healthy has to go beyond just a clinical room, just the exam room,” Smith said. “It’s got to go back into their communities.”
Anyone in crisis can seek confidential and free help by contacting the 988 Suicide & Crisis Lifeline by texting or calling 988 or reaching out online at 988lifeline.org.
CLEVELAND – Violent blows or jolts to the head can cause traumatic brain injury (TBI), and there are currently about five million people in the U.S. living with chronic neurodegeneration and related impairments due to TBI. In addition to cognitive and mental health impairment, chronic neurodegeneration may also contribute to why TBI increases the risk of age-related neurodegenerative diseases, such as Alzheimer’s or Parkinson’s disease. It could also play a role in chronic traumatic encephalopathy (CTE).
Due to the lack of understanding of why acute TBI transitions into chronic neurodegeneration, however, there are currently no treatments that protect patients from this outcome. Now, University Hospitals (UH) and Case Western Reserve University researchers have moved a step closer to finding answers in a study recently published in Cell Reports Medicine.
“We started with the hypothesis that TBI might pathologically impair the balance of mitochondrial fission and fusion,” explained Preethy S. Sridharan, PhD, lead author of the study. “The normal homeostatic balance of mitochondrial fission and fusion is how mitochondria consistently produce enough energy for the cell while also sequestering and disposing damaged parts. Given the very high energy demands of the brain, this is particularly important for brain health across our lifespan.”
The process is governed by the interaction of two cellular proteins: Fis1 and Drp1. It was previously shown that other neurodegenerative diseases, including Alzheimer’s disease (AD) and Huntington’s disease, display pathologically elevated mitochondrial fission due to elevated expression of Drp1. Here, the research team discovered that mitochondrial fission is pathologically elevated in mouse and human TBI as well, but that it is caused by increased expression of Fis1, rather than Drp1.
They next tested whether pharmacologically reducing excessive mitochondrial fission for only two weeks after TBI, by administering a small peptide agent named P110 that blocks the interaction of Fis1 and Drp1, might halt this process and protect the brain. P110 was previously discovered and developed by co-senior author, Xin Qi, PhD, the Jeanette M. and Joseph S. Silber Professor of Brain Sciences in the CWRU Department of Physiology and Biophysics and Co-Director of the CWRU Center for Mitochondrial Research and Therapeutics.
“Brief P110 treatment during the acute time period after TBI permanently normalized mitochondrial fission / fusion and prevented subsequent harm to the brain, including oxidative damage, blood-brain barrier deterioration, axonal degeneration, and cognitive impairment, 17 months later. This is equivalent to many decades in people,” explained Andrew A. Pieper, MD, PhD, senior author of the study and Director of the Brain Health Medicines Center of the Harrington Discovery Institute at UH. “The same treatment administered much later, however, had no protective effect. Thus, there is a critical time window after TBI wherein this treatment can be effective.”
Dr. Pieper also holds the Morley-Mather Chair in Neuropsychiatry at UH and the CWRU Rebecca E. Barchas, MD, DLFAPA, University Professorship in Translational Psychiatry. He additionally serves as Psychiatrist and Investigator in the Louis Stokes VA Geriatric Research Education and Clinical Center (GRECC).
The team hopes that P110 or a related compound will be tested clinically in acute TBI patients. “Next steps in the basic science research, on the other hand, involve further utilization of this model to yield additional new insights into understanding the pathophysiology and treatment opportunities for this important problem,” explained Dr. Qi.
In addition to extending their investigation to additional different preclinical models of TBI, the research team also plans to investigate whether the mechanism they discovered could play a role in why TBI accelerates AD. They speculate that the combination of increasing two components of the same system (increased Fis1 in TBI and increased Drp1 in AD) could cause a synergistic deleterious effect that significantly advances the development and severity of AD after patients have experienced a TBI.
___
This study was supported by The Valour Foundation.
Sridharan, Preethy S. et al. “Acutely blocking excessive mitochondrial fission prevents chronic neurodegeneration after traumatic brain injury.” Cell Reports Medicine.DOI: 10.1016/j.xcrm.2024.101715